
ViroLIEgy
16 Apr 2024 | 12:42 am
Blinded by Pseudoscience
My recent exchanges with defenders of virology and germ theory on Twitter have really opened my eyes as to how entrenched the indoctrination has become and how critical thinking skills and logic have been entirely wiped away from many people. Not only is there a fundamental misunderstanding of the dogma that these individuals are attempting to defend, they do not even have a working knowledge as to what science is or how to distinguish real science from fake science, i.e. pseudoscience. They are at a complete loss as to what makes up the scientific method and why this process must be adhered to in order for the knowledge gained to be considered science. While this may be forgivable for the layperson, many of these people I interact with consider themselves scientists and educators. They are microbiologists, immunologists, researchers, and teachers. Not having an understanding as to what science is or is not supposed to be at that level is unforgivable. However, when one understands that the educational system, through the use of memorization and the repeated regurgitation of pseudoscientific rhetoric, is set up to churn out industry slaves who lack the ability to think critically and logically, it begins to make sense.
Perhaps these individuals are too close and far too heavily invested into the allure of the pseudoscience they've been taught as true science that they cannot see the forest for the trees. I know I have been a victim of such a scenario myself. When I started out as a personal trainer, I was a firm believer in utilizing supplements for health and personal wellness gains. I regularly read up on the latest whey protein and creatine products on the market. I was well-versed in the "wonders" of the various new formulas based upon the magazines that I read and was heavily influenced by; the very magazines that are financed by the supplement industry whose products were being promoted within these publications.
With my first personal training job, the gym I worked for provided further training and certification in nutrition and supplementation by bringing in a company that sold its own line of supplements. The spokesperson would come in and do intricate presentations with lots of excitement and energy about their products. We were taught how their products were made and how they were far superior to those found at the supermarkets, as their line was created using pharmaceutical manufacturing processes. This company proudly proclaimed that they were GMP (Good Manufacturing Practices) certified, while the competitors were selling unregulated mystery compounds. We were sold on how their products would not only help our clients lose weight but also gain lean muscle mass and improved health.
I was a parrot for the company, hocking their supplements to my clients while making grandiose promises and claims about the potential benefits. I cited studies that I did not read and promoted benefits that were scientifically unproven. When clients complained that the multivitamin we sold turned their urine blindingly bright neon yellow, I regurgitated the company line that this was natural and meant that the body was absorbing the vitamins it needed while excreting those it could not use. This radioactive-looking urine was supposed to be the sign to the client that the product was "working." We also sold protein cookies and brownies that were meant to replace the Chips Ahoy and Ho-Ho's people were consuming as part of an unhealthy lifestyle. If clients complained that they had made all the necessary dietary changes and were still gaining weight while eating the protein cookies and brownies, I reassured them that these were the "better bad food choices," as I had been instructed to do, and that the clients were to practice moderation. I was a good soldier and I did as I was told. I made lots of money selling these products and I regularly used them myself. I was a true believer and remained as such until I left the company. Only when I stepped out of that environment and took a wider view of what I was doing, did I finally realize the errors of my ways.

Thus, it may be easier for those of us outside of the industry to examine it critically, and to do our due diligence in truly understanding the problems in the field, than those who are currently plugged into and benefitting from the system. In order to examine virology and its related fields honestly, I needed to let go of my preconceived ideas as to what "viruses" are as well as what led to disease. I had to refresh my understanding of what science is and what it is not. I needed a way to gauge the evidence presented in order to hold it accountable to an agreed upon standard. Understanding and utilizing these standards and criteria in order to critique the evidence is what sets those of us who are investigating these fields apart from those who are unwilling to examine the evidence critically themselves.
When I first started my journey into uncovering the fraud of virology, the barometer that I utilized to determine whether the evidence was valid or not was Koch's Postulates. This criterion was devised in 1890 by German bacteriologist Robert Koch and it includes four logical requirements that are necessary to be satisfied in order to claim that a specific microbe causes disease. They are as follows:
- The microorganism must be found in abundance in all organisms suffering from the disease, but should not be found in healthy organisms.
- The microorganism must be isolated from a diseased organism and grown in pure culture.
- The cultured microorganism should cause disease when introduced into a healthy organism.
- The microorganism must be reisolated from the inoculated, diseased experimental host and identified as being identical to the original specific causative agent.
This is definitely a logical criterion that should be satisfied if one is to claim that a microbe causes disease. However, many virology defenders angrily claim that the Postulates were developed specifically for bacteria and are thus not relevant for "viruses." They also claim that Koch eventually abandoned some of his requirements in order to fudge…er, I mean, "confirm" his findings that certain bacteria are pathogenic. This is despite the fact that the WHO and many virologists disagree and state that the Postulates must be satisfied in order to prove a microbe is pathogenic. In any case, I explained why these arguments against the Postulates are irrelevant here.
While Koch's Postulates are still valid logical requirements, there is a much better method that must be adhered to first in order to establish and claim a causative relationship. We can side-step the angry rantings of those tearing down the Postulates that Koch built by sticking to the methods that built science. These steps are known as the scientific method. As there is quite a bit of confusion over the scientific method in those who claim to be scientists themselves, I want to explore why this process is absolutely essential as the barometer to distinguish science from pseudoscience and why it is necessary to hold virology and its related fields to this standard. Hopefully, through this exploration, it will be easier to understand what the true purpose of science is, why the scientific method is the only measure that is required, and how to identify pseudoscience that is fraudulently masquerading as the real deal.

To begin with, we need to examine what the purpose of science truly is. When investigating this topic, it will become readily apparent that there are many definitions for what science is supposed to be. However, we can see that there are core tenets shared in all of them. According to Merriam-Webster, science is defined as such:
knowledge or a system of knowledge covering general truths or the operation of general laws especially as obtained and tested through scientific method
https://www.merriam-webster.com/dictionary/science
In Webster's New Collegiate Dictionary, the phrase "concerned with the physical world" was added:
knowledge covering general truths of the operation of general laws, esp. as obtained and tested through scientific method [and] concerned with the physical world.
https://scienceline.ucsb.edu/getkey.php?key=1408
According to Vocabulary.com, science is an empirical field, i.e. based on observation or experience:
Science is an "empirical" field, that is, it develops a body of knowledge by observing things and performing experiments. The meticulous process of gathering and analyzing data is called the "scientific method," and we sometimes use science to describe the knowledge we already have.
https://www.vocabulary.com/dictionary/science
According to BiologyOnline.com, the body of knowledge is systemized and gained from observation and experience:
A systematized body of knowledge in the form of hypotheses, theories, principles, models or laws that have been conclusively drawn from observed or verifiable facts or from experimental findings gained basically from the application of the scientific method.
https://www.biologyonline.com/dictionary/science
Finally, from the Science Council, the understanding of the natural and social world through evidence is added:

As can be seen from these definitions, science is the systemized acquisition of knowledge about the physical and natural world that is based upon the evidence gained through observation and experimentation. The systematic process utilized to generate the evidence which leads to this knowledge is known as the scientific method, a series of logical steps that were designed to test a hypothesis in order to obtain a general understanding of what causes an observed natural phenomenon. The scientific method is primarily concerned with either establishing or disproving a relationship between two variables. While many in the sciences try to dispute that there should be a strict adherence to this method, it is clear that it is vital to adhere to this process in order to establish knowledge that is considered scientific. Even Wikipedia understands that science requires the use of the scientific method:
Scientific research involves using the scientific method, which seeks to objectively explain the events of nature in a reproducible way.[167]
https://en.m.wikipedia.org/wiki/Science

The steps that make up this method may vary a little depending on the source but there are core elements that are regularly found in all outlines. These include observing a phenomenon, establishing a hypothesis, testing the hypothesis through experimentation, and examination of the data to validate/invalidate the hypothesis. My favorite outline of the scientific method further expands upon all of these core elements by providing a few more details:
- Observe a natural phenomenon
- Alternative hypothesis
- Independent variable (the presumed cause)
- Dependent variable (the observed effect)
- Control variables
- Null hypothesis
- Test/experiment
- Analyze the observation/data
- Validate/invalidate hypothesis
Let's examine each of these 6 steps briefly in order to provide greater clarity.
 1. Observe a Natural Phenomenon
1. Observe a Natural Phenomenon
This may be the most controversial of the core steps as people try to argue over what is considered a phenomenon. However, there should be no confusion when we define the word as it is most commonly understood; a phenomenon is an observable fact or event. A natural phenomenon is an observable fact or event that occurs in nature that is not man-made nor influenced or manufactured by human engineering or intervention. The cause or explanation of this observation is in question, which leads one to start to investigate the matter scientifically in order to provide an explanation. Observing a natural phenomenon is usually done through the senses either by sight, sound, taste, touch, or smell. However, some phenomena are unable to be detected directly through the senses and require enhancement through the aid of technology such as microscopes, telescopes, stethoscopes, etc. Some examples of natural phenomena that are not man-made include lightning/thunder, volcanic eruptions, weather, decomposition, earthquakes, fire, etc. It is through the observation of the phenomenon that the necessary questions are asked in order to move into the next step in the process, forming a hypothesis.
2. Alternative HypothesisThe hypothesis is the foundation of the scientific method. It is an educated guess as to a possible explanation for what has caused the observed phenomenon. In order to have a valid hypothesis, there are two crucial elements that must be defined from the very start. These are the independent and dependent variables. The independent variable (IV) is the presumed cause of the effect that was observed. The IV must actually exist and be able to be varied and manipulated throughout experimentation to see what affects it may have, if any. It cannot be the end-result of the experiment. The dependent variable (DV), on the other hand, is the effect that was observed and that the researcher is looking to identify the root cause for. Unlike the IV, the DV cannot be directly manipulated as it is entirely dependent upon the manipulation of the IV.
Once both variables are identified, a hypothesis can be formulated. This is written as an if-then statement and drawn up as a possible explanation as to what may happen to be discovered upon experimentation. An example would look like this:
"If I water my plant every day, then it will grow."
In this example, the water is the IV while the growth rate of the plant is the DV. Along with these variables, there are other factors that must be identified as well, known as control variables. These are the factors that may influence the outcome of the experiment. In our example, these could include the amount of sunlight, the type of soil, the time of day, the temperature, the weather, indoor or outdoor environment, etc. Control variables must be accounted for and must remain unchanged throughout the course of the experiment. This is to ensure that any effect attributed to the IV was actually a result of the IV alone and not due to other confounding factors.
3. Null HypothesisAn absolutely essential component of the hypothesis is that it must be falsifiable, meaning that it can be proven wrong. This is why one must also be able to establish a null hypothesis, which assumes that there is no relationship between the IV and DV. In other words, it is the exact opposite of the alternate hypothesis. Using our earlier example, it would be written simply as such:
"If I water my plant every day, it will not grow (or it may grow less or may die)."
It is this very concept of falsifiability that is a hallmark of true science. If one is repeatedly unable to falsify the alternate hypothesis, this is a very strong indicator that the results are indeed valid scientifically.
4. Test/ExperimentIt is at this stage where the real heart of science takes place. In order for the knowledge gained to be considered scientific, the hypothesis must be testable through experimentation. This is where the hypothesis will either be proven or disproven in regard to the causal relationship between the IV and the DV. The experiment must focus on only changing one variable at a time and must be repeated numerous times. The main experiment will coincide with control experiments to ensure that the hypothesized results are only seen with the experimental group. In order to be considered a success, the expected results must not be seen in the control group and must be reproduced more than once.
Going back to our water and plant example, we could plant seeds in two identical pots with the same soil. We would need to figure out how much water we want to use and then water our experimental pot daily while our control pot receives water once a week. As the plants grow, the height of each plant would be measured to see if the amount of water had any effect on the growth of the plant.
5. Analyze the Observation/DataAfter experimenting, the data is collected and ready for analysis in order to confirm or reject the hypothesis. This is rather self-explanatory. In our plant scenario, the heights would be measured to see what kind of difference may have been noticed. Did the experimental plant grow faster? Or perhaps daily watering resulted in over-watering and the death of the plant. How did the results compare with the control? Which plant fared better overall? Once completed, the experiments can be run again, if validated, in order to see if the results are repeatable and reproducible.
6. Validate/Invalidate HypothesisThis is another self-explanatory step. Either the experiment produced the intended result, thus confirming the alternative hypothesis, or it did not, thus confirming the null hypothesis. If it did not confirm the alternative hypothesis, then it is back to the drawing board to either come up with a new hypothesis and/or examine the variables which may have impacted the experimental results.
Once the basics of the scientific method are understood, it should be easy to apply this criterion to any of the sciences in order to see how they stack up. The scientific method is the barometer that I have relied upon in order to critique virology and its related fields. We can use virology as an example for how this can be done. Starting with the observation of a natural phenomenon, the best that virologists can do is point to shared symptoms in sick patients. However, they can do nothing more than guess as to what could be the potential cause as, beyond speculating that fluids from coughing and sneezing may transfer disease, virologists cannot witness disease being transferred from person-to-person. In fact, many experiments outright debunked the possibility that the fluids could transmit disease, most famously outlined during the Spanish flu with the experiments performed by Milton Rosenau in 1918. As researchers could not pin many instances of disease on a bacterial agent (if any), they had to dream up the idea that something smaller than the bacteria was hiding within the fluids of a sick patient. Unfortunately for virology, this is where the entire field encounters its fatal flaw. Virologists have never been able to directly demonstrate the existence of "viruses" either within the fluids of sick patients or within the environment. They are unable to purify (free of contaminants, pollutants, foreign materials) and isolate (separate from everything else) the assumed "viral" particles from the host and the environment. As they have never been able to identify their independent variable nor do they have the IV on hand from the very beginning, there is no ability to create a valid hypothesis. Without establishing the existence of the IV and without the creation of a testable and falsifiable hypothesis, virology cannot even get to the experimental stage in order to generate the data to verify their non-existent and untestable hypothesis. Thus, virology fails to even get off the ground in adhering to the scientific method.
However, this has not stopped virologists from experimenting anyway and claiming that their results, created from these fraudulent endeavors, indirectly prove the existence of the entity that they cannot directly show within the fluids. This is in large part thanks to the cell culture method that was devised in 1954 by John Franklin Enders as he attempted to "isolate" the measles "virus." As virology could not find their IV (the "virus") within the fluids or the environment, they decided to create their IV by taking the fluids of a sick patient and mixing them with monkey kidney cells in a Petri dish full of kidney-toxic antibiotics, antifungals, fetal bovine serum, minimal nutrients, and other chemicals and ingredients. In doing so, they created their own DV called the cytopathogenic effect (CPE), which is the breakdown of the cell into smaller pieces as it dies from being poisoned. Virologists then claim that the effect that they experimentally create and observe was directly caused by the "virus" that was never shown to exist before the experiment ever took place.
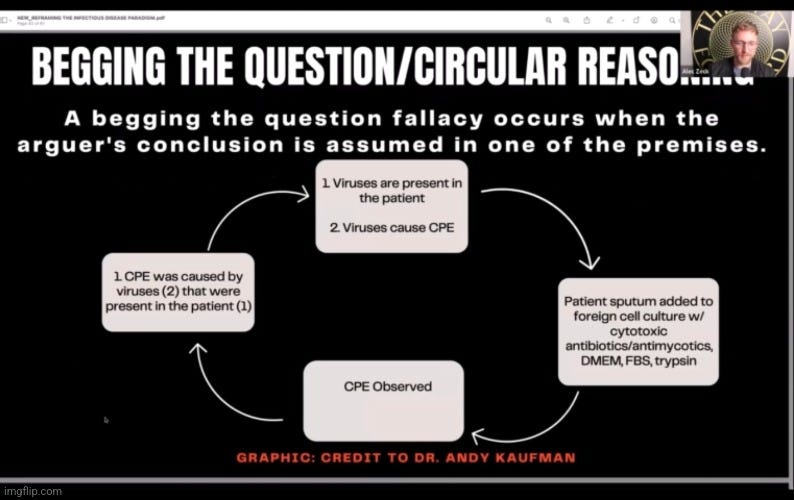
It should hopefully be very clear how this series of events are the exact opposite of the scientific method. The "virus" is assumed to be present from the start but is never on hand as an IV that can be varied and manipulated. The CPE generated in the Petri dish is not a natural phenomenon that was observed, but is instead a lab creation. There is no possible way to establish a valid hypothesis as both the IV and the DV do not exist in a natural state from the start. They are lab-created artifacts that only exist after experimentation and never before. Proper controls are regularly ignored and when they are performed, the results show that no "virus" is ever necessary in order to get the same cytopathogenic effect. There are many known examples which can bring about this effect such as bacteria, parasites, antibiotics and antifungals, the age of the cell, contamination, the act of passaging, etc. This knowledge has not stopped virologists from claiming that the results generated from these unscientific methods are scientific. However, they are not scientific at all. In fact, these results are the exact opposite. They are pseudoscience.

Pseudoscience is exactly what it sounds like: fake science. The problem is that pseudoscience can look and act just like the real thing to anyone who is unfamiliar with how to identify it. Fortunately, there are some telltale characteristics of pseudoscience that can be used to set it apart, such as:
- Making up explanations to fit any observed outcomes.
- The "virus" caused the CPE or, if not present, there was a non-CPE producing "virus"
- The misuse of the commonly held definitions for words.
- Purification and isolation = mixing many contaminants together in a petri dish
- The use of rescue device explanations for contradictory results.
- Asymptomatic carriers of disease
- Sample was taken too early to show antibodies
- Claims presented as scientifically established when they are not.
- "SARS-COV-2" is the etiologic agent of a new disease called "Covid-19"
For further insight into what makes up pseudoscience, I want to share a few excerpts from an article I came across discussing this topic. In this first excerpt, what we will see is that, while pseudoscience may appear logical to an extent, it is ultimately unfalsifiable. This is by design, as shown by virology and its many escape clauses:
Non-science Pseudoscience"Non-science may be logical, or even "true" by certain criteria. But if something is unobservable, untestable, unpredictable, or inconsistent, or if it exists outside the natural world and does not abide by natural laws, then it is beyond the scope of scientific inquiry. It cannot be tested and therefore predictions or explanations regarding its nature, behavior, cause, or effect cannot be verified nor can they be falsified. For example, many cultures and religions around the world describe the concept of a human soul or spirit. However, since that is not something Science is able to directly test or observe, then it is considered non-science (i.e., not scientific).
The author notes that an area of study is beyond the scientific scope if it is:
- Unobservable
- Untestable
- Unpredictable
- Inconsistent
- Exists outside the natural world and does not abide by natural laws
Think back to how the "virus" itself is unobservable, that the results can be inconsistent and are regularly explained away, and that, as a non-living entity, a "virus" is outside the natural world and does not abide by the natural laws. The "virus" belongs to what immunologist Paul Ehrlich described as "the realm of the invisible." Or, as most would call it, the imagination.

In this next excerpt, the author goes on to note that if it cannot be tested, "predictions or explanations regarding its nature, behavior, cause, or effect cannot be verified nor can they be falsified." He provides an excellent example from popular ghost hunting shows as to how technology and the derived measurements can be used to claim the presence of something that may not exist in reality but only as a belief. It is a great analogy for virology and its related fields:
"But, Mr. Franklin!" I can hear you saying, "I've watched shows on TV where ghost hunters used all sorts of sophisticated scientific instruments to document the paranormal!" Indeed, hucksters often try to dress-up non-science with scientific-seeming sights and sounds. They explore so-called "haunted" houses with infrared thermometers, EMF meters, anemometers, and other instruments like those shown below, on the belief that ghosts cause fluctuations in electromagnetic fields, cold spots, or breezes. The problem is, however, that none of these claims can be falsified, meaning they cannot be disproven. If a ghost hunting team fails to record any significant data, then they may claim the ghost didn't show up or wasn't powerful enough. On the other hand, any variation in data is taken as evidence that suggests the presence of a ghost! There's no way to disprove the existence of ghosts beyond pointing out the lack of strong evidence."
https://franklinscience.weebly.com/science-vs-non-science.html
Essentially, what the above information is pointing out is that, in order to be considered scientific, the evidence gained must have been obtained through the adherence to the scientific method. If it is derived in any other manner and is unable to be observed, tested, and falsified, it is pseudoscience. Many have argued over such a simplified distinction, but this is backed up by various definitions of what pseudoscience is.
According to Oxford Languages, pseudoscience is defined as such:
a collection of beliefs or practices mistakenly regarded as being based on scientific method.
Oxford Languages and Google – English
According to BiologyOnline.com:
Any body of knowledge, methodology, belief, or practice purported to be scientific but which fails to comply with the scientific method, lacks supporting evidence, or cannot be tested in practice or in principle.
https://www.biologyonline.com/dictionary/pseudoscience
According to TechTarget.com:
Pseudoscience is a proposition, a finding or a system of explanation that is presented as science but that lacks the essential rigor of the scientific method.
https://www.google.com/amp/s/www.techtarget.com/whatis/definition/pseudoscience%3famp=1
According to Study.com:
Pseudosciences often appear to be a genuine science, but they do not follow the scientific method.
https://study.com/learn/lesson/pseudoscience-overview-examples.html
And once again, even Wikipedia understands that without the scientific method, it isn't science:
Pseudoscience consists of statements, beliefs, or practices that claim to be both scientific and factual but are incompatible with the scientific method.
https://en.m.wikipedia.org/wiki/Pseudoscience
We see a very familiar common denominator in all of these definitions:
Pseudoscience does not adhere to the scientific method.It truly is that simple. If you understand the method and you know what you are looking for, that is all you need in order to be able to distinguish between real and fake science. Thus, we can easily see that if something is claiming to be science, but it does not adhere to the scientific method, it is, by definition, pseudoscience. As shown above, virology does not follow the scientific method and is pseudoscience. One can easily apply this criterion to the related fields surrounding virology (immunology, genomics, epidemiology, etc.) and come to the same conclusion.
A major problem in the sciences right now, which has inevitably led to the current issues regarding the reproducibility crisis and the inability to trust much of what is considered scientific research, is a lack of standardization. While the scientific method exists as a means to weed out fake science and it is meant to be adhered to for this very reason, it is regularly ignored or even disparaged, either by those in the scientific community or in the media. It is clear that many of the papers that are published today do not follow the very process that was established long ago to ensure the validity of the evidence being accepted as scientific. When these criteria are applied to what has been published, it becomes alarming how much scientific evidence is, in actuality, pseudoscientific evidence falsely presenting as the real deal.
Why are people in the sciences so ready and willing to abandon the scientific method in order to engage in and defend pseudoscience? Perhaps it is because the scientific method simply is not being taught as well as it should be. In an exchange on Twitter with a person who was in a teaching position, it was immediately clear that they did not understand the scientific method at all nor its importance. When I pressed for information that showed that the foundational evidence for the topic we were discussing actually adhered to the scientific method, I was provided a link to the textbook Lehninger Principles of Biochemistry 9th Edition as proof that the work discussed adhered to the scientific method. However, I immediately found that the textbook made no such claim. In fact, in the over 1100 pages of principles related to biochemistry, the scientific method was only ever mentioned twice and never in connection with the work we discussed. These were the two sole mentions:
"The scientific method sometimes advances an issue slowly, and a truly insightful experiment can be difficult to design."
And:
"A key feature of the scientific method, as Albert Einstein once summarized it, is "No amount of experimentation can ever prove me right; a single experiment can prove me wrong."
In the end, this individual admitted that the foundational paper we discussed did not adhere to the scientific method and was thus, by definition, pseudoscience. However, this acknowledgment did not deter their belief in the slightest, as it was suggested that later research eventually did follow the scientific method. No evidence was ever presented backing up this claim. This should be shocking to anyone with an ounce of intellectual honesty. If the people in these teaching positions do not understand the scientific method, easily accept pseudoscientific findings, and teach from textbooks that do not even provide a rudimentary explanation of what it entails, how can we expect those who are the future of the scientific research to uphold these necessary standards? How can we trust that the papers of tomorrow are scientifically sound rather than cleverly disguised pseudoscience? How can we accept the evidence that has come before for which these future papers are to be built on top of? It is time to demand that the evidence being presented as science adheres to and upholds the necessary standards that were established to flush out fraudulent results. It is time to challenge scientists to demonstrate how their given fields live up to this standard. We must use the scientific method as the barometer to examine the foundational papers in a given field in order to see what passes muster as true scientific knowledge and what ultimately falls into the category of pseudoscience. I imagine many will be surprised at how little can actually be classified as science when all is said and done. It is time for the evidence that is being sold as science to be held to the established scientific standard as it should have been done from the very beginning.
This article originally appeared on ViroLIEgy's Antiviral Substack.
29 Mar 2024 | 2:41 pm
The “Virus” Concept
You go through narrow-pored clay filters, which hold back all bacteria, easily pass through and you have they are not yet visible with the best microscopes, including the ultramicroscope can do. We must infer their existence because they represent various human, animal and plant diseases. It's a very special strange fact that we are dealing with these microorganisms that are completely invisible to us can operate in exactly the same way as with pure cultures of bacteria.
-Robert Koch
https://tinyurl.com/yth9wx87
The above quote was taken from one of German bacteriologist Robert Koch's final speeches, the inaugural address at the Academy of Sciences on July 1, 1909. He passed away almost a year later on May 27th, 1910. At the time, Koch acknowledged his belief that there were entities that were invisible even under the best microscopes. As they were invisible and represented certain diseases, their existence had to be inferred from evidence that was similar to that seen in the studies on bacteria. In other words, if a bacterium was sought after and failed to be identified as the causative agent of a disease, it was acceptable to blame an unseen culprit. The diseases that could not be linked to bacteria and required the invisible scapegoat to keep the germ theory alive included measles, scarlet fever, smallpox, rabies, influenza, yellow fever and cattle plague. According to Field's Virology textbook, the concept of the invisible "virus" was born once the researchers realized that they were unable to satisfy Koch's Postulates, the criteria considered absolutely necessary to fulfill in order to prove that microbes cause disease:
"These studies formalized some of Jacob Henle's original ideas in what are now termed Koch's postulates for defining whether an organism was indeed the causative agent of a disease. These postulates state that (a) the organism must be regularly found in the lesions of the disease, (b) the organism must be isolated in pure culture, (c) inoculation of such a pure culture of organisms into a host should initiate the disease, and (d) the organism must be recovered once again from the lesions of the host. By the end of the 19th century, these concepts became the dominant paradigm of medical microbiology. They outlined an experimental method to be used in all situations. It was only when these rules broke down and failed to yield a causative agent that the concept of a virus was born."

Researchers began to claim that, if they used filters that were small enough to keep known bacteria out, and the resulting fluids after filtration resulted in symptoms of disease in animals, this was evidence that something smaller than a bacteria existed within the fluids that caused the disease. This gave rise to the term "filterable viruses." The Field's Virology textbook goes on to explain that, once this idea of "filterable viruses" was accepted, a procedure was created in order to find them. This is the technique known as the cell culture that was established by John Franklin Enders in 1954, nearly 60 years after the idea of the "filterable virus" was conjured up. Virologists had to rely on factors such as the size of the pore of the filters, whether there was a reaction to chemical agents (alchohol and ether), and whether or not they observed cytopathogenic effects (CPE) in the cell culture as indirect evidence (i.e. evidence that does not prove a fact but can be used to infer that the fact exists) in order to claim that the invisible entities were within the fluids. As virologists could not see the entities that they assumed to be present, they had to rely on faith that they were there:
"Once the concept of a filterable virus took hold, this experimental procedure was applied to many diseased tissues. Filterable agents, unable to be seen in a light microscope, that replicate only in living animal tissue were found. There were truly some surprises, such as a virus—yellow fever virus—transmitted by a mosquito vector (122), specific visible pathologic inclusion bodies (viruses) in infected tissue (80,116), and even viral agents that can "cause cancer" (43,123). Throughout this early time period (1900–1930), a wide variety of viruses were found (see Table 1) and characterized with regard to their size (using the different pore sizes of filters), resistance to chemical or physical agents (e.g., alcohol, ether), and pathogenic effects. Just based on these properties, it became clear that viruses were a very diverse group of agents. Some were even observable in the light microscope (vaccinia in dark-field optics). Some were inactivated by ether, whereas others were not. The range of viral diseases affected every tissue type. Viruses gave rise to chronic or acute disease; they were persistent agents or recurred in a periodic fashion. Viruses might cause cellular destruction or induce cellular proliferation. For the early virologists, unable to see their agents in a light microscope and often confused by this great diversity, there had to be an element of faith in their studies. In 1912, S. B. Wolbach, an American pathologist, remarked, "It is quite possible that when our knowledge of filterable viruses is more complete, our conception of living matter will change considerably, and that we shall cease to attempt to classify the filterable viruses as animal or plant"
The concept of the invisible "virus" was used in order to explain away any evidence that contradicted the idea that microbes were the cause of disease once it was realized that Koch's logic-based requirements could not be satisfied. Virologists were emboldened to bend the rules as Koch himself regularly did so as well. He knew that it was often impossible to induce disease in animals in order to claim a microbe as the causative agent, as evidenced by his troubles with cholera. Unfortunately, instead of realizing that his Postulates worked as designed by disproving microbes as causative agents of disease, Koch allowed for logic to be bent in order to keep the germ theory alive. This was admitted in Alfred Grafe's "A History of Experimental Virology:"
"Since Koch knew, after his 1884 experience with cholera, that it was often impossible to induce a disease experimentally in animals and yet not harbour the slightest doubt about the germ theory, he augmented these guidelines. His thoughts on the implications of the regular and exclusive occurrence of bacteria in infectious diseases without a possible animal experimental trial was reflected in his own words:
"Our contention is likely justified, even at this point, that if only the first two requirements for proof are fulfilled … the causal relationship of parasite to the disease is validly established."
Nevertheless, it is essential to explain how it was possible to arrive at Koch's postulates in a manner which contradicted Koch himself."
As admitted by Grafe, Koch completely contradicted himself by allowing for a microbe to be claimed as a causative agent even if the disease was not recreated experimentally. Previously, Koch claimed that this was the only possibility of providing direct proof of causality:
"The only possibility of providing a direct proof that comma bacilli cause cholera is by animal experiments. One should show that cholera can be generated experimentally by comma bacilli."
Koch, R. (1987f). Lecture cholera question [1884]. In Essays of Robert Koch. Praeger
-Robert Koch
Koch also eventually allowed for the microbe to be identified as the causative agent in cases where the disease did not occur (i.e. in the healthy). Thus, depending on the situation, Koch abandoned and contradicted his own logical postulates in order to fit evidence to the germ theory of disease so that it could be kept afloat in the face of contradictory evidence and the inability to fulfill his criteria. The creation of the invisible "virus" was the latest effort to try and plug the holes in the sinking germ theory ship.
Tobacco Mosaic "Virus" (TMV)
Tobacco mosaic "virus" is regarded as the first "virus" ever to be discovered, officially ushering in the era of virology. This is a disease that is supposed to result in spotting discoloration of the leaves of the plant. However, the symptoms experienced (mottling, yellowing, leaf curling, stunted growth, and necrosis) by the plant are said to be very dependent on the host plant, the age of the infected plant, the environmental conditions, and even the genetic background of the plant. These influences on the disease process were relegated to co-factors as the search for a specific microbe was pursued. Due to the inability to cultivate a bacterial agent that could be associated with the disease, the idea floated about that there was an invisible entity, originally regarded as a poison rather than actual particles, that passed through filters small enough to keep out bacteria.
With TMV, the two men often credited with the discovery of the first "virus" are the aforementioned Dmitri Ivanovski and Martinus Beijerinck. In 1892, Ivanovski attempted to discover the microbial cause of the disease by crushing the leaves of diseased plants and passing the resulting leaf sludge through various filters. He claimed that the filtered juices, when inoculated onto healthy plants, produced the same disease as seen in nature. This usually involved scraping or injecting the plant and/or leaves, thus damaging them, putting the filtered juice on the leaves, and then monitoring the leaves to see if the spotted disease occurred. Ivanovski's 1892 paper "Considering the Tobacco Mosaic Disease in Plants" is considered the first report on the filterability of "viruses." However, there are no details on his experimental methods within the paper, and all that is provided are his own claims that passing the crushed plant leaves through a Chamberland filter, said to hold back bacteria and fungi, still produced disease:
"that the sap of leaves attacked by the mosaic disease retains its infectious qualities even after filtration through Chamberland filter candles."
According to Alfred Grafe's "A History of Experimental Virology," Ivanovski concluded that the agent must be either a specific bacterium or a specific toxin, although he could find neither. Even upon further experimentation by Ivanovski in 1903, and after assessing the results of his experiments on the tobacco mosaic disease agent, Grafe concluded:
"it is not possible to find evidence on the nature of the causative agent. Ivanovski did not offer proof in his experiments or in his illustrations that the causal agent was a bacterium. Furthermore, there is no indication of his having suspected a new type of causative agent."
Thus, it is easy to see that Ivanovski could not identify any agent—bacterial, fungal, or "viral"—and relied on lab-created experimental effects, such as filterability, in order to claim that an invisible "infectious agent" was present. He remained convinced that, despite being unable to cultivate any bacterium along with repeated failures to produce evidence, the causal agent was an unculturable bacterium that was too small to be retained on the Chamberland filters or to be detected by light microscopy. Regarding the idea that the causative agent could be something other than bacterial, Ivanovski claimed that he:
"succeeded in evoking the disease by inoculation of a bacterial culture, which strengthened my hope that the entire problem will be solved without such a bold hypothesis."
Ivanovsky, D. 1899 Ueber die Mosaikkrankheit der Tabaksp£anze. Centbl. Bakteriol. 5, 250^254
This was Ivanovski's response to the idea proposed by Martinus Beijerinck a few years later in 1898 that the "filterable agent" of the tobacco mosaic disease was not bacterial, but rather something like what we now think of as a "virus," which he called the Contagium vivum fluidum, i.e. contagious living fluid. In his work, Beijerinck repeated a similar process to Ivanovski and attempted to filter the juices of diseased plants and then inoculcate the healthy plants with injections of the filtered fluids. The leafs that were "infected" occurred directly above the "wound" created by the syringe, which is not a natural route of exposure or "infection." In order to speed up the disease, all one had to do was create a deeper wound and insert diseased material. Interestingly, Beijerinck discussed how formalin used to sterilize the syringe was extremely toxic to the tobacco plant and that one had to ensure that no traces of formalin remained in the syringe when used for experiments. He even mentioned that the disease from the artificial inoculation was different from the disease that is seen naturally in plants:
Concerning a Contagium vivum fluidum as cause of the spot disease of tobacco leaves"The quantity of candle filtrate necessary for infection is extremely small. A small drop put into the right place in the plant with a Pravaz syringe can infect numerous leaves and branches. If these diseased parts are extracted, an infinite number of healthy plants may be inoculated and infected from this sap, from which we draw the conclusion that the contagium, although fluid, reproduces itself in the living plant."
"Often (perhaps always) the leaf that first becomes diseased is situated directly above the wound left by the infecting needle. If the place of infection was closely circumscribed, for example to a single shallow puncture of the needle with the Pravaz syringe, the second diseased leaf, in a s leaf position, may be exactly the ninth above the first one to become diseased."
"If one wishes to convince oneself in the shortest possible time of the virulence of the contagium it is best to deeply wound with a knife the youngest part of the stem below the terminal bud, which still may be easily treated without injury, and to place into the wound a piece of fresh, diseased tissue. The newly formed leaves will then plainly show the first traces of the disease after ten to twelve days; after three weeks the disease symptom is clearly distinguishable, even to the layman."
"In any case, one must be sure that the last traces of Formalin have completely evaporated from the syringe before using it again, for it has become apparent that Formalin is very poisonous for the tissues of the tobacco plant, much more so than to the virus itself."
"Although most of the dead tissue spots develop in the manner described near or in the dark-green fields near the veins, the origin of some of them remains uncertain; apparently, they also may develop in the yellow spots. The symptoms in the tobacco fields are usually not of as great an intensity as in artificial infection, especially the blistery outgrowth of the dark-green parts on the leaf blade is entirely lacking. In contrast to this, the necrosis and drying of leaf spots were not observed in some of the greenhouse plants.
With artificial injection of fresh extracted sap, or with inoculation with diseased tissue the disease may reach a higher stage of intensity than I have as yet observed under natural conditions. I mean the abnormal tissues of the newly formed leaves (Plate I b, c, d, Plate II, fig. 4 and 5). This is no doubt connected with the quantity of infectious material used for the experiment. Therefore, it is much easier to produce leaf monstrostities with fresh extracted juice than with the Bougie filtrate, since, as has been remarked earlier, more of the latter must be injected m order to obtain the same effect, which certainly is remarkable for a contagium that increases through growth."

Being unable to produce the disease exactly as seen in nature along with the unnatural route of "infection" by wounding plants and injecting them from a syringe should be enough to disqualify Beijerinck's experimental results and conclusions. However, like the virology papers that came afterward, no proper controls were ever performed by Beijerinck with fluids from healthy plants treated and inoculated in the same manner, thus further disqualifying his findings. According to Grafe, Beijerinck's ideas about the causative agent, which he regarded as a liquid toxin rather than infectious particles, were disregarded, rejected, and no longer discussed at the time:
"Beijerinck's concepts were equally disregarded! As early as 1898, he had assumed in his reflections on colloid chemistry that "virus" might be a living, liquid contagium, and commented that it was probably taken up by a living cell, in which it then reproduced. Although protein-like crystals, i.e. organized biological material, had been known since Hartig's description ofthem in 1856, a liquid contagium hardly fitted into the concept of an infectious pathogen at that time. In short, Beijerinck's idea met with rejection and his model of multiplication was discussed no further."
Interestingly, when attempting to determine a "founder of virology," Grafe mentioned that even though Beijerinck's ideas were close to the concept of the "virus" as it is known today, he made no attempt, theoretical or experimental, to prove or even to defend his hypothesis that the infectious agent was a contagious living fluid. In other words, all Beijerinck had was an unproven hypothesis, i.e. an assumption, which essentially disqualifies him. Grafe equally questioned Ivanovski as "the founder of virology" as, in order to even consider him, all of Ivanovski's published findings would need to be disregarded. Grafe stated that Ivanovski did not follow the established rules of etiological experiments and arrived at false conclusions. Thus, the two men that are most often credited as having discovered the first "virus," are completely discredited as neither were able to identify any causative agent:
The literature often cites someone as the "founder" of virology. Since it is customary – for non-scientific reasons – to associate the word "founding" with one particular person, in the case of virology such a contention can only be defended superficially. When Beijerinck is mentioned, the scales tip in his favour because his ideas at the close of the 19th century sound to us so modern. Speaking against him is the fact that he made no attempt, theoretical or experimental, to prove or even to defend his hypothesis of a Contagium vivum fluidum and its intracellular reproduction. To declare Ivanovski "father of virology" can only be credible if we disregard his publications. He did not observe the established rules for etiological experiments, and consequently arrived at false conclusions. In his opinion, the pathogen for TMD was a bacteria which could be photographed. On the other hand, no one can deny that he was the first to filter the causative agent of a plant disease, not discounting Mayer's use of filter paper in 1880."
Foot-and-Mouth Disease (FMD)
Foot-and-mouth disease (FMD) is a set of symptoms said to first be identified as a specific disease in the late 1800s. According to the Cornell College of Veterinary Medicine, FMD is characterized by fever and blister-like lesions followed by erosions on the tongue and lips, in the mouth, on the teats, and between the hooves. Most animals recover, but the disease "results in a weakened state, loss of weight, and reduced production of milk and meat." It is said to afflict mostly animals such as cows, pigs, sheep, goats, deer, and others with divided hooves, but it has been claimed to affect humans as well. As this disease was affecting livestock and causing economic loss, there was a major push by the Prussian government to find a vaccine against it. This ultimately led to the appointment of Friedrich Loeffler, a pupil of Robert Koch, to head up a Commission established n 1897 seeking to create a vaccine against the disease. He was under considerable political and economic pressure to create a vaccine as quickly as possible, even without identifying any specific cause.
The results from Loeffler's Commission were reported in four separate documents between April 17, 1897 and August 12, 1898. In the last of Loeffler's four reports, he called attention to the fact that there were several bacterial and other amoeba-like microbes claimed by various researchers to be the causative agents of FMD. He spent a considerable amount of time at the beginning of his report discussing the work of Drs. Siegel and Bussenius, who had claimed to have discovered a specific bacterium in man and animals that had died of the foot-and-mouth disease. The doctors claimed to have even recreated the foot-and-mouth disease experimentally in animals using pure cultures of their bacterium. However, when Loeffler's Commission attempted to grow the same bacterium from the blood of sickened animals, the results were considered negative, even though certain bacteria were grown. These were claimed to be either micrococci or pseudo-diphtheria bacilli that were said to be impurities due to contamination.
The Commission also attempted to recreate Drs. Siegels and Bussenius' animal experiments, even though they had the excuse at the ready for any experimental results that may have confirmed the findings. They stated that experiments of this sort "might easily lead to a false conclusion, since the disease might be conveyed to the inoculated animals by the attendants, or even by the members of the Commission themselves." In other words, any positive results may not be due to a bacterium but by accidental spread of the "actual causative agent" by those involved. Attempts were made to "infect" calves by feeding them 50 ccm. of two-day old bouillon or by inoculation from scarification (involves scratching, etching, burning/branding, or superficially cutting) on the upper and lower lips. This was said to be the same method used to "infect" animals with foot-and-mouth disease lymph. The sucking calves became ill with high fever and symptoms of intestinal affection, with one killed while the other died "naturally." The bacilli were found in the blood and spleen of both animals. However, as neither animal had the characteristic lesions on the mouth or hooves, the experiment was considered negative.
Due to concerns by Drs. Siegel and Bussenius that not enough time was given for the lesions to develop, three more calves were experimented on. However, the amount of bouillon that was used with the calves was reduced from 50 ccm to 2 ccm in one calf and 5 ccm in the two remaining calves. This produced similar results, and, once again, the experiments were considered negative. Loeffler concluded that Drs. Siegel and Bussenius had an "interesting and remarkable pathogenic organism" that was "capable of setting up severe intestinal disease." However, it was decided not to be the cause of foot-and-mouth disease. Somehow, these results were also used to disregard the findings of a bacterial cause by numerous other researchers (Nosotti, Klein, Schotteluis, Kurth, Nissen, Starcovici, Furtuna, and Stutzer) as well. Even claims put forward by Piana, Fiorenti, Behla, and Jurgens of small protoplasmic structures with distinct amoeboid movements as causative agents were disregarded in favor of Loeffler's own unidentifiable and invisible agent:
Report of the Commission for the Investigation of Foot-and-Mouth Disease at the Institute for Infectious Diseases, Berlin."Nevertheless the Commission considered it necessary to submit to examination a particular species of bacterium which had been found by Drs Siegel and Bussenius in alleged fatal cases of foot-and-mouth disease in the human subject, and also in cases of the same disease in animals, and this appeared to be the more necessary because these authors had alleged that they had been able to produce typical foot-and-mouth disease in calves and pigs with pure culture of their bacillus."
"Inasmuch as, according to the views of its discoverers, the bacillus is mainly found in the blood of recently attacked animals, although frequently only in very small numbers, special attention was always directed to examination of the blood. In five cases blood was taken from the jugular vein of recently attacked animals by means of a sterile trocar, and collected in sterile Erlenmeyer flasks; blood was also taken from the heart of two calves which had been killed at the height of the disease immediately after development of vesicles. Large quantities of the blood were used to inoculate bouillon, nutrient agar, and nutrient bouillon, the flasks being then placed in the incubator. In the great majority of cases the flasks thus inoculated remained permanently sterile, but in a few of them micrococci, and in some others bacilli, developed. Most of the latter belonged to the group of pseudo-diphtheria bacilli, and had not the most remote resemblance to the bacillus of Siegel and Bussenius. They were obviously accidental impurities which had been obtained from the skin of the animals in taking the blood.
These negative results of experiment are in contradiction with the positive assertion of the authors named, that they had succeeded in producing the typical disease with their bacillus; nevertheless the Commission considered it advisable to afford them an opportunity to demonstrate the experimental production of the disease with the bacillus. The Commission were mindful of the fact that experiments of this sort might easily lead to a false conclusion, since the disease might be conveyed to the inoculated animals by the attendants, or even by the members of the Commission themselves, who were almost daily brought mto contact with animals suffering from foot-and-mouth disease."
"Inasmuch as it was possible that the bacillus of Seigel and Bussenius might have lost some of its virulence from long cultivation in nutrient gelatine, at the desire of these two gentlemen an attempt was made to infect the two sucking calves by pouring about 50 ccm. of a two-days-old bouillon culture of the bacillus into the mouth of each animal. At the same time, however, two yearlings were inoculated by scarification on the upper and lower lips in the same manner as one proceeds in infecting animals with foot-and-mouth disease lymph. In the case of the yearlings the material employed was a fresh culture of agar, and a large quantity of the culture was also rubbed on the mouth of these two animals, so that an infection of the intestine was also made possible.
On the following day the sucking calves were already ill, with high fever and symptoms of intestinal affection. One of them was killed while very ill on the third day, and the other died in the course of the following night. In both of these animals the bacilli were found in the blood and spleen, and especially in the much swollen mesenteric glands, as well as in contents of the intestines. Their presence in these positions was demonstrable by microscopic and cultural examination. Neither of the animals had lesions in the mouth or on the feet, such as are characteristic of the disease in question. On the contrary, they were affected with a severe enteritis.
With a two-days-old bouillon culture started from the heart blood of the above calf in which death resulted naturally, three new animals were infected at the instigation of Drs Seigel and Bussenius, in order to induce a less acute form of the disease, and thus to give time for the production of the characteristic lesions. One of these was a sucking calf and it received 2 ccm. into the mouth. The second animal was a three-months-old calf, and the third a yearling, and each of these received 5 ccm. into the mouth. On the following day the sucking calf was already the subject of high fever and profuse diarrhrea, and it died on the fourth day. The post-mortem examination showed practically the same conditions as in the above-mentioned calves."
"The three-months-old calf became ill on the second day, being also attacked with high fever and profuse diarrhrea. Subsequently, however, it recovered, though its temperature remained for a long time over 41° C. Both the inoculated yearlings, and also the one infected by feeding, sickened on the fourth day, with rather high fever and profuse diarrhrea. The fever lasted from two to four days, and as it declined the diarrhrea also abated. During fourteen days' observatIon none of the animals showed any symptoms of foot-and-mouth disease.
From these experiments it follows that the bacillus of Seigel and Bussenius, although an interesting and remarkable pathogenic organism, capable of setting up severe intestinal disease, is not the cause of foot-and-mouth disease.
From the results of the investigations above described it may also be concluded that the bacteria found by other observers-Nosotti, Klein, Schotteluis, Kurth, Nissen, Starcovici, Furtuna, and Stutzer, in cases of foot-and-mouth disease, did not represent the causal agent of the infection.
There still remained for investigation the claims of certain observers who have described, not bacteria, but small protoplasmic structures with distinct amoeboid movements, as the cause of the disease. Claims of this sort have been put forward by Piana, Fiorenti, Behla, and Jurgens."

According to Loeffler, the only animals that he could "infect" with any certainty with his "agent" were calves. Experiments with twenty-two pigs only resulted in eight "infections." He admitted that there were no successes in eight attempts with sheep, and only one out of eight goats became "infected." He also tried, via inoculation into the mucous membrane of the mouth or the limbs, intraperitoneal injection, or through the feeding with fresh materials, to "infect" 30 rabbits, 14 guinea-pigs, 3 dogs, 4 cats, 5 rats, 10 house mice, 10 field mice, 6 hens, and 6 pigeons, but all of these attempts failed.
Loeffler stated that the way to "infect" animals was with rubbing the mouths with materials moistened in the fluids of deceased animals. However, he admitted that this did not always result in "infections." In one instance, only 9 of 17 animals were said to be "infected" in this manner after three days of attempts. The disease was said to be successfully experimentally transmitted to two yearlings and 13 calves by rubbing a drop of lymph on the slightly scarified mucous membrane of the upper and lower lips. In other words, they roughed up the mucous membranes in some way (cutting, sanding, burning, etc.) and then rubbed lymph into the wound. If blisters formed after abrasive scarification and the rubbing of unclean materials into the wounds, it was considered a success. No attention is paid to the very acts of scarification and rubbing being the cause of the blisters rather than any invisible entity. In the great majority of the cases, the disease only attacked the areas wounded around the mouth and not the feet of the calves.
Transmission of the Disease to Different Species of Animals.-The only animals that we have been able to infect experimentally with certainty are cattle (2) or calves (13). Out of twenty-two attempts to infect pigs only eight were successful. There was no success in eight attempts with sheep, and only one out of the same number with goats. Attempts were also made to infect 30 rabbits, 14 guinea-pigs, 3 dogs, 4 cats, 5 rats, 10 house mice, 10 field mice, 6 hens, and 6 pigeons, but the attempts failed, whether they took the form of inoculation into the mucous membrane of the mouth or into the limbs, intraperitoneal injection, or feeding with fresh materials.
Mode of Infection.-According to experience, in adult cattle and calves infection follows when materials moistened with fresh slaver from diseased animals, such as towels, sponges, or wisps of straw, are used to rub the mouth; but even in this way infection does not always follow with certainty. For example, in one instance only nine out of seventeen animals which it was sought to infect in this way on each of three successive days in the same building contracted the disease. The disease was experimentally transmitted to two yearlings and 13 calves by rubbing a drop of lymph on the slightly scarified mucous membrane of the upper and lower lips. The vesicles developed not only at the places scarified but also in their neighbourhood, on the palate and tongue. In the case of the yearlings vesicles developed on the feet, but in the great majority of cases the disease did not attack the feet in the calves. It was observed that the vesicles formed on the feet one or two days after the disease had shown itself in the mouth. On the second or third day after experimental infection the temperature rose 1° or 1 1/2°, and in the course of the next three days it fell to the normal. The formation of vesicles set in from the first to the third day, generally on the second day, after inoculation. In the case of ten oxen inoculated in the skin of the back or on the posterior aspect of the thigh, no local lesion was produced, and up to the fifth day after inoculation none of the animals appeared to have contracted the disease. Unfortunately this experiment was vitiated by the fact that three days after the inoculation in the skin the owner had also attempted to infect the animals, so as to get rid of the disease as quickly as possible. After that the animals developed the symptoms of foot-and-mouth disease, but it was impossible to determine whether this was the result of the first or the second attempt to infect them."
The material said to be "infectious" were materials taken from the vesicles. Attempts to "infect" with the serum of the blood from diseased animals failed to produce disease. The most certain method of "infection" was considered the introduction of the invisible "virus" hiding within the contents of vesicles into the blood stream. Loeffler also claimed success by injecting the "virus" into the peritoneal cavity and into the muscles, as well as rubbing the materials into the mucous membrane of the mouth after wounding by pricking. Inoculations into and under the skin proved uncertain:
"Infective Material.–The contents of freshly developed vesicles have been found to be the most certainly effective material for infection. Serum of blood taken from the jugular vein of diseased animals during the period of vesicle formation, and subcutaneously injected in quantities of from 10 to 14 ccm., did not produce the disease in three calves. Experiments regarding the infectivity of the urine and feces of diseased animals have not yet been carried out."
Method of Infecion.-Through numerous comparative experiments it has been ascertained that the most certain method of infection is the introduction into the blood stream of the virus found in the contents of vesicles. Success has also attended the introduction of the virus into the peritoneal cavity, injection into the muscles, and rubbing of it into the mucous membrane of the mouth after wounding by pricking. On the contrary, inoculations into and under the skin have proved uncertain. Both of these appear to be effective only when at the same time the virus is introduced into a blood vessel. From the moment that the temperature begins to rise till the development of the local symptoms of the disease, the virus circulates in the blood stream, but it disappears from the blood after the development of the local lesions. The disease could be conveyed to healthy animals with from 50 to 100 ccm. of blood taken from the jugular vein of an animal twenty to twenty-eight hours after its inoculation."
In attempts to determine the microbe via injections of filtered and unfiltered lymph into animals, both the filtrate and the control animals showed typical signs of illness. When "fresh lymph fluid" was used, the animals treated with the filtered lymph always became affected in the same way as the control animals treated with unfiltered lymph. This led Loeffler to two possibilities: either the "germ-free" filtered lymph contained an "extraordinarily active poison," or there was an undiscoverable agent that was so small that it could pass through the pores of a filter that bacteria could not pass through:
"The result of these injections was somewhat surprising. The animals which received the filtrate contracted the disease in the same time as control animals which had received a corresponding quantity of unfiltered lymph, and they all showed typical symptoms of the disease, with high fever and the development of vesicles in the mouth and on the feet. It appeared as if the activity of the lymph had not been affected by the filtration. In order to be quite certain regarding this point the experiments were several times repeated on a large number of calves and pigs. When fresh lymph was used the results were always the same, the animals treated with the filtered lymph always becoming affected in a quite typical way, just like the control animals treated with unfiltered lymph.
How was this striking fact to be explained? Two alternative explanations offered themselves- either the germ-free filtered lymph contained in solution some extraordinarily active poison, or the hitherto undiscoverable agent of the disease was so small that it could pass through the pores of a filter which will certainly keep back the smallest of the known bacteria. If the first explanation is the correct one, the soluble poison must be an amazingly active one."

According to Grafe, Loeffler's FMD reports resulted in a "pathogen" that was "not identifiable under the microscope" and was one "belonging to a new type of causal agent." The Commision decided that, in order to develop a vaccine, it was desirable—but not absolutely necessary—to identify the causative agent. Loeffler and his colleagues concluded that the FMD "pathogen" belonged to a group of the smallest organisms, but Grafe pointed out that they did so "without any clear demarcation to the bacteria." Grafe stated that the criterion of a "filterable virus" was considered significant by Loeffler as "a laboratory index but not for the characterization of a new causative organism." In other words, Loeffler did not clearly distinguish between bacteria and his "filterable agent," and only used the term to classify his unidentifiable agent rather than claiming that a new entity existed.
A 1999 paper by H. P. Schmiedebach provides even more details on Loeffler's Commission and their work, highlighting many other reasons for why their results can be disregarded. The primary goal of the Comission was to find a vaccine. The identification of the "causative agent" was considered a side effect from these efforts. However, as it was not possible to actually visualize the "virus," Koch's Postulates could not be completely employed. Schmiedebach noted that Loeffler's work de-emphasised the theoretical and the scientific requirements while the political, practical and public context ultimately determined the experimental strategy as well as the focal points of his research. Therefore, Loeffler could not present scientifically derived evidence for the existence of his unidentifiable agent.
Loeffler excused his inability to directly identify his agent by guessing that it must be smaller than 0.1 um, thus even the best microscopes of the time would not be able to visualize it. There were no means by way of microscopy or any other methods that the Commission could utilize to identify the invisible microbe. Oddly enough, in 1903, Loeffler declared Koch's Postulates as the decisive goal to be met in order to prove a microorganism causes disease. Ironically, without being able to visualize the entity nor grow it in pure culture, Loeffler failed to satisfy this "decisive attainment" with regard to the identification of the FMD microbe:
The Prussian State and microbiological research – Friedrich Loeffler and his approach to the "invisible" virus"The research programme concerning FMD, which was initiated by political authorities, was primarily aimed at the development of an effective vaccine but led, as a side-effect, to the virus itself. Nonetheless, it was not possible to find a way to visualize the supposed virus and thus Koch's postulates could not be completely employed. Loeffler emphasized the practical side of his research activities, which to some extent de-emphasised the theoretical and scientific requirements. The political, practical and public context determined the experimental strategy and the focal points of his research."
"These calculations, based on a mechanical view without consideration of possible metabolic activities, brought him to the conviction that there existed a germ of very small size that could pass through common filters. Nonetheless, he could not present scientifically derived evidence for the existence of that small germ. Loeffler was fully aware of this epistemological dilemma. In his record he added an explanation for the impossibility of seeing this very tiny germ. He referred to correspondence with Professor Abbe in Jena who was an authority of the highest reputation regarding microscopic techniques. Loeffler discussed with him the limitations of microscope performance. If the supposed germ of FMD had a size of only about 0.1 um, even the best immersion techniques of that day could not made this virus visible. According to Loeffler, this would be best explanation for the fruitless attempts to discover the germ by microscopic investigation. Although this was a very pessimistic view, he tried to turn the tables and offered a perspective concerning the possible discovery of a large number of other germs that could not be identified at that time. In connection with the necessity of future studies on that problem, the commission also requested for the grant of new financial support from the government."
"The commission could not identify the supposed microbe by microscope nor was it possible to make it visible by any other methods. However, there were some scientific requirements to be fulfilled in order to accept a supposed germ as the causative agent for a disease. In 1903 Loeffler himself wrote on the occasion of Koch's 60th birthday about the scientific foundations of the newly emerged discipline of bacteriology and declared the development of "Koch's Postulates" as a decisive attainment. While Koch had mentioned four postulates in 1890, Loeffler referred only to three:
1. "Constant evidence of the concerned organism in all cases of the disease;
2. isolation of the pathogen in a pure culture that had to be cleaned of all corpuscular elements of the sick individual;
3. generation (Wiedererzeugung) of the disease anew by reliable pure cultures."
I will not discuss the differences from Koch's original formulation but we must evaluate whether Loeffler himself undertook any steps to employ these three postulates in the case of FMD and which, if any, he employed. As we have already seen, two very successful methods, microscopy and culture, failed with regard to the identification of the microbe."
Interestingly, Schmiedebach noted that, in 1907, the Prussian government accused Loeffler of spreading FMD via his experiments, and he was shut down for two years. Loeffler did not publish any papers describing the nature of his "virus" and he performed no experiments to prove any theories in the field. Loeffler was tied to the bacteriological field as taught to him by his mentor Koch, and he saw no convincing reasons to reject his teachings:
"In 1907, Loeffler was confronted with numerous difficulties. Since 1902, he had been using a farm in Greifswald for his trials. In 1907, the Prussian Minister of Agricultural Affairs accused Loeffler of being responsible for the dissemination of FMD in the region of Greifswald. Loeffler's experiments at this farm were seen as the main cause for the spread of the disease."
"Following this, and considering the heavy pressure, it is not surprising that Loeffler was not in the contemplative mood required to publish sophisticated articles about the nature of the virus and to perform experiments to prove one or the other theory in this field. In addition, he was adherent to the bacteriological paradigm that had presented many successful discoveries up to that time and he did not see any convincing reason to reject this concept. Considering all the ramifications of his work, his research strategy, despite all the remaining questions and the epistemological uncertainty, becomes more comprehensible."
https://pubmed.ncbi.nlm.nih.gov/10470267/

According to chapter 3 of Grafe's A History of Virology, Loeffler's methods were the model for others who investigated "filterable viruses" at the time. Even though the term included the word "virus," the opinion prevailed for over three decades after it came into use that the "filterable virus" was merely a very small bacteria. Nothing was undertaken experimentally to investigate other hypotheses that differentiated the "filterable viruses" from being anything other than small bacteria.
Thus, it is abundantly clear that, like Ivanovski and Beijerinck before him, Loeffler did not discover any new causative organism. Even though he considered Koch's logic-based criteria as decisive in proving a microorganism as the cause of disease, Loeffler was unable to satisfy Koch's Postulates for his "filterable virus." He was unable to culture any microorganism nor could he visualize one. His experimental "infections" resulted in contradictory results depending on the species of animals and the route of "infection." Reminiscent of Ivanovski and Beijerinck's own methods, no attention was given to the fact that the best results came from unnatural routes of exposure that required wounding the host. With Ivanovski and Beijerinck, this meant cutting the plant while injecting materials into the resulting hole. For Loeffler, this meant scarifying the lips, mouths, and mucous membranes of the animal and rubbing diseased materials into the wounds. These methods do not reflect nature in any shape or form.
Regardless, none of the three researchers credited with identifying the "filterable viruses" for the first time provided valid scientific evidence to support such a claim as to the discovery of a new entity. Dmitri Ivanoski's methods were ill-defined and he did not follow the established rules of etiological experiments, leading to false conclusions. He did not provide any evidence on the nature of his "causative agent," nor any proof in his experiments or in his illustrations that the "agent" was a bacterium or anything else. Nevertheless, he believed that his "agent" was nothing more than a small bacterium.
Matrinus Beijerinck made no attempt, theoretical or experimental, to prove or defend his hypothesis that his "infectious agent" was a contagious living fluid. His experimental "infections" resulted in disease that was not the same as that seen in nature and his work did not involve proper scientific controls. His idea of a liquid toxin as the causative agent rather than the "infectious particles" that "viruses" are known as today, was disregarded, rejected, and no longer discussed at the time.
Friedrich Loeffler de-emphasised the theoretical and the scientific requirements of his work and allowed the political, practical and public context to determine the experimental strategy as well as the focal points of his research. He could not provide any scientifically-derived evidence for his "agent" and yet, he still believed that what he had was a small invisible bacterium as he never made any attempt to classify his findings in regard to the discovery of a new entity.
Clearly, the "filterable virus" is nothing more than an imaginary concept that was established by bacteriologists who failed to associate any bacteria as a causative agent through the satisfaction of Koch's Postulates. These researchers created artificial and experimental disease through unscientific and unnatural methods, thus leading them to believe that there was an invisible agent that was responsible rather than the disease being a direct result of the damaging methods used. Had the proper controls been carried out utilizing fluids taken from healthy hosts or those suffering other diseases that were treated in the same manner, these researchers would have realized, just as the Prussian government did with Loeffler, that it was the experiments themselves bringing about disease, not any "filterable viruses." Instead, an invisible scapegoat was conjured up in order to explain away contradictory results and to mask up the pseudoscientific findings, allowing the germ theory of disease to live another day.
This article originally appeared on ViroLIEgy's Antiviral Substack.
15 Mar 2024 | 2:15 pm
The Infectious Myth Busted Part 7: The Common Cold Vacation
It's a safe bet to say that, at one moment in time or another, we have all reached that level of complete physical and mental exhaustion where we feel that we have reached a breaking point. For some, it is due to being overworked with long arduous hours and seemingly never-ending shifts. For others, it is due to continual sleepless nights after the arrival of a new child. It could be a combination of the two, having to raise one or more kids while juggling multiple jobs and struggling to pay off the ever-increasing debt and monthly bills in order to make the ends meet. The numerous stressors of everyday life may be all that is required to bring us to this moment in time where we feel the need to escape. There are various different scenarios that can occur that will bring about this burning desire within us to get away from it all so that we can have a reprieve. Thus, when the opportunity arises to hit the time-out button so that we can pause our regularly scheduled lives for a moment for a much needed vacation, most of us will jump on and seize the opportunity.
Beginning in the late 1940s, over 20,000 people who needed to get away from the hardships of life were presented with just such a golden opportunity thanks to the Common Cold Unit at Salisbury in Wiltshire. This was due to the desperate need for the researchers to acquire human guinea pigs…er, I mean, volunteers…so that they could study the common cold "virus." In order to get these volunteers, ads were placed in print promising a cheap and comfortable 10-day holiday where everything was free and people would receive a modest compensation for their troubles. It was sold to the public as the perfect getaway as well as a chance to make a difference, with one ad stating: "Free 10 Day Autumn or Winter Break: You May Not Win A Nobel Prize, But You Could Help Find a Cure for the Common Cold." Researchers would go on TV and radio promoting the ammentities offered, even targeting honeymooners looking for a relaxing time. All that the volunteers had to do in order to partake in this paid vacation was subject themselves to experiments with fluids which may or may not contain a common cold "virus." The ads worked, and as stated in a 1982 profile piece in The New York Times, unemployed workers, students writing theses, civil servants using up excess leave, housewives and thrill seekers came calling in order to secure their reservations for a luxurious stay at Salisbury.

This decades-long experiment is where we get our "knowledge" about the common cold from. As it is such an important moment in the history of virology, one that is unlikely to ever be replicated today due to "ethical" concerns, let's examine the origins of this event. Let's investigate what exactly went on at this facility and find out whether they were truly successful in their endeavors. Let's see if we can pinpoint exactly why people were so eager to risk "infection" with a "virus" to the point that the facility was over-subscribed with a waiting list of willing participants excited to have their very own common cold vacation. At the end, it will be clear why these people decided to book return trips to Salisbury over and over again.
The Origin of the Common Cold…Unit.
In 1941, during the height of the second world war, Harvard University and the American Red Cross decided to gift to Britain both an epidemiological team as well as a wartime "infectious" disease hospital that it had set up for the British military. According to virologist David Tyrrell, who had worked for the Rockefeller Institute and eventually ran the facility for the majority of its time in operation, funds were raised from individual donors and foundations to send a team equipped to do field studies as well as set up a laboratory and a hospital containing 125 beds to serve civilians. The hospital was planned and its buildings and equipment were said to be ordered "off the shelf" in Washington. It was originally envisioned as a stopgap to deal with feared epidemics of cholera and typhoid outbreaks arising from the bombing of infrastructures during the war. However, the dreaded epidemics never occurred, and from 1942 to 1945, it was given to the US on the premise that the hospital would be relinquished once the war was over. During this time, it was utilized to assemble, store and type the enormous supplies of blood needed for the war effort until it was officially declared over in 1945 and the facility was abandoned.
However, the facility didn't remain abandoned for long as English virologist Dr. Christopher Andrewes, who was working to convince the British Medical Research Council to fund a long term study investigating the common cold and related respiratory diseases, decided that the hospital offered the perfect set-up to undertake such research. Dr. Andrewes approached the Medical Research Council for funds to set up and run a research laboratory, which it ultimately approved for the investigation into the cause of common colds and how they spread. The facility was refurbished and the laboratory was equipped so that the first intake of volunteers were able to arrive in July of 1946.
Although he was successful in establishing his new facility to study the common cold "virus," there was a bit of a problem for Dr. Andrewes and his team. According to his 1950 paper Adventures Among Viruses. III. The Puzzle of the Common Cold, while their main objective was to find a way of studying the common cold without the use of human volunteers, they could not cultivate or see any "virus." Dr. Andrewes lamented, "if only we could cultivate and, if possible, see the virus, or produce infection in some convenient small animal," that it would make them happy, profitable, and busy for dozens of years. Dr. Andrewes pointed out that his crew "have not satisfied ourselves that we can cultivate the virus by any one of many available technics in fertile hens' eggs." Not only were they unable to grow any "virus," the crew attempted – in vain – to produce colds in mice, rats, guinea pigs, cotton rats, rabbits, voles, hamsters, gray squirrels, hedgehogs, ferrets, kittens, pigs, green monkeys, red patas monkeys, capuchin monkeys, baboons and a sooty mangabey. In fact, they attempted to recover "virus" from several species in order to "reinfect" human beings, but this was constantly met without success. Dr. Andrewes admitted that they had, at that time, failed to meet their primary objective.
While he noted that they had not succeeded, Dr. Andrewes did, as any good virologist does, point out the unreliable indirect evidence that they had accumulated to try and claim the existence and presence of a "virus." Even though they could not see a "virus," he claimed that filtration procedures had given them some "knowledge" as to the size of the invisible "virus," stating that it was less than half the size of the "influenza virus." However, he noted that the size could range anywhere from 20 to 50 mu. Commenting on using the electron microscope to image the "virus," Dr. Andrewes pointed out that success depended on getting "virus" particles in a state of reasonable abundance and purity, which was not possible at that time. He admitted that the influenza "virus" could not be imaged until they started culturing in embryonic fluids in fertile hens eggs:
"Some knowledge has been gained of the physical properties of the virus. Filtration through graded collodion membranes indicates a particle size rather less than that of influenza virus. This is about 0.1 a or 100 mu across. The experiment shows the difficulty in interpreting results obtained on small groups of subjects. Clearly, the virus has passed the membranes with pores 120 to 140 mu across, but are we to lay stress on the one definite cold produced from a 57 to 68 mu filtrate? If this is genuine the probable size of the virus is around 20 mu or less. If it is a false result, the probable size would be regarded as about 50 mu. The question is of some importance for it would be well worth while attempting with refined optical methods to photograph a virus 50 mu across. One would have much less hope of success with something of half that diameter. I should say something at this point about the prospects of photographing a virus such as this. It is often asked whether the cold virus cannot be depicted by the aid of the electron microscope. Almost certainly it is within the range of sizes accessible to this instrument, but all success in this field depends on first learning how to obtain virus particles in a state of reasonable abundance and purity. That tame, amenable, domestic creature, the influenza virus, was never photographed satisfactorily until we had first learned how to grow it in quantity in embryonic fluids of fertile eggs. So we are back again against the dire need for a way of growing the virus of the common cold."

The CCU researchers were to use these filtered secretions presumed to contain the invisible "virus" in an attempt to "infect" volunteers. If a volunteer experienced symptoms associated with a cold, it would be assumed that a "virus" caused the cold. Ironically, Dr. Andrewes had hoped that his report on their studies "made it clear how much about colds we don't know, and how slow our increase of knowledge is bound to be, unless someone can find a trustworthy method of laboratory study." While he hoped that the day would come soon, he felt at that time that the problem of studying the common cold was "obscured by the mists of folklore, superstitution and pseudoscience."
The inability of Dr. Andrewes, and that of his partner Dr. Alick Isaacs, to grow cold "viruses" in the laboratory led them to the realization that they needed to recruit as many human volunteers as they could get if they were going to study a "virus" that they could not find or see. This ultimately led to a marketing push to sell the public on participating in an unusual vacation opportunity in order to acquire the necessary human guinea pigs. The New York Times reported that, at Dr. Andrewes opening press conference, "he made headlines by suggesting that honeymooners might take advantage of the facilities by becoming experimental subjects." If the crop of human guinea pigs began to thin out, Dr. Andrewes would make a round of appearances on radio and on television to promote the wonderful facility. The main attraction was the price of the stay as it was entirely free, and volunteers would actually earn money for participating. Harvard footed the bill, paying for all travel expenses and supplying $2.80 a day for pocket money. The volunteers would stay in furnished rooms in one of the converted barracks, with each unit of two to three rooms sharing a living room and a kitchen with a refrigerator, a teapot, and a toaster. Warm meals were prepared and delivered to the doors of the volunteers in thermos containers. They had access to a television and a radio-cassette player for music. They had different activities to pass the time such as building jigsaw puzzles, playing board games such as Monopoly or Scrabble, reading books from the library, and using the telephone to make calls. They even had the use of a miniature-golf course, paddle-tennis court or a pool table for recreational activities, as well as the beautiful outdoor countryside of the Salisbury Plains that they could take leisurely strolls outside in nature. All they had to do was stay 10 yards (30 feet) apart at all times, as that was apparently the magic number that the "virus" could not travel beyond.


The facility was advertised in newspapers and magazines as "an unusual holiday opportunity in an attractive part of the countryside, at no cost and with financial reimbursement." The volunteers were actually encouraged to spread the word amongst friends and family, and they had the option to reapply every six months. In fact, it was considered such a nice stay that one couple alone logged 21 visits at the facility.
As Dr. Andrewes noted, opening an all-expenses paid vacation facility to experiment on human guinea pigs was not the main objective of their work, which was to find a way of studying the common cold without, or with very little, use of human volunteers. The inability to grow the "virus" along with the failures of every effort to produce commercially viable vaccines or antivirals resulted in the facility almost being closed on a number of occasions. The lack of success in their endeavors ultimately led to the appointment of Rockefeller virologist David Tyrrell, who considered himself a "reluctant young virologist," as the head of the unit to oversee the research in 1957. Tyrell's appointment was seen as a last-ditch effort to culture the "virus" assumed to be responsible for the common cold in order to forestall the closure of the unit. Fortunately for the CCU, this gambit "miraculously" paid off as in 1960, the year that the unit was scheduled for closure, Tyrrell's crew published three papers claiming to "isolate" the common cold "virus." Thus, the Common Cold Unit survived for another 30 years.
Tyrrell's Tenure
During David Tyrell's tenure, new methods were created to "grow" the "viruses" that they would use to try and "infect" the volunteers with. This involved the researchers experimenting with both tissue and organ cultures in attempts to establish successful "infections." The first method that they utilized to "grow" a "virus" required human embryo kidney cells that were incubated at 33°C and passaged twice, which resulted in no cytopathogenic effects (CPE), the pattern of cell death claimed by virologists to be a sign that a "virus" is present, resulting in a "successful" culture. The medium was then modified in order to allow for serial passaging and to "speed up" the development of the CPE that the researchers wanted to see, as the original "rhinovirus" cultures took 25 days and at least one passage in order to develop. In other words, they manipulated the cultures until they were able to kill the cell faster and claim success:
"However it is my guess that the development of general methods using tissue cultures, and later organ cultures, of cells, was generally faster and more logical at the Unit where we were able to combine the use of new culture techniques with the inoculation of volunteers to indicate that a cold-producing agent was growing to even a limited extent. We first found a method for propagating many different 'cold' (actually rhino-)-viruses in roller tube cultures of human embryo kidney cells at 33°C for two passages, without a cytopathic effect (CPE) (Tyrrell et al., 1960). The medium was modified, first to allow serial passage and the development of interference, and then to allow a rapid CPE to occur (Tyrrell and Parsons, 1960; Hitchcock and Tyrrell, 1960). Others later found more convenient susceptible cells."
Interestingly, Tyrrell admitted that the human embryo tissues that they utilized were not adequately checked for all possible contaminants. He also stated that they would use monkey kidney cells on occasions and that, as they were unaware of "non-cytopathogenic agents," the researchers did not look to ensure that these cells were free of all possible contaminants. In other words, the researchers were not using purified preparations that contained only the presumed "viral" particles:
"Extensive use was made of human embryo tissue – this was obtained from patients with no clinical history or evidence of infection and was handled in a 'clean' area. However it was tested only for bacterial and fungal infection before administration to volunteers. Furthermore on some occasions virus propagated in monkey kidney cells was used, and although the cultures were tested for haemadsorbing and cytopathic agents, we did not know
about non-cytopathic organisms such as SV40 and so did not test for them."
These same organ culture methods were utilized by Tyrrell in 1965 in order to "isolate" the very first "coronavirus" known as B814, which oddly enough, mysteriously disappeared in the early 1970s. In his paper, nasal washings were immediately stored in phosphate-buffered saline and bacteriological nutrient broth. The washings were then transferred into organ cultures of 14-to-22-week-old fetuses mixed with medium 199 and sodium bicarbonate. The medium was changed daily for two days in order to "grow" the "virus." Interestingly, it was said that the organ culture fluids produced more frequent and severe colds in volunteers than just the unpurified nasal washings alone. Dr. Andrewes had noted in 1950 that the broth and saline that they used as controls never produced colds, but other substances utilized for the same purposes, such as suspensions of normal egg-yolk sac, produced mild colds in small numbers. Thus, the more foreign, unpurified and contaminated the source is, the more cold symptoms that are seemingly produced. Dr. Andrewes also noted how culturing can easily fool the researchers into believing that they have a "virus" when nothing is there, stating "one time we thought we had successfully cultivated cold virus in eggs, but tests with more uninoculated eggs revealed that we had added one more to our unique collection of will-o'-the-wisps."
Regardless of having more "success" when utilizing cultured soups to inoculate the volunteers with, Tyrrell would later note that the results with culture fluids were regularly unable to be repeated. He spoke of how they needed to manipulate the cultures in order to get the best results, such as using human cells rather than monkey cells, incubating at 33°C instead of 37°C, and using the synthetic medium 199. If they attempted too many passages, the results when trying to "infect" volunteers were always negative:
"We did seem to produce colds with culture fluids but the results would not repeat regularly, and testing the components took ages. There was evidence that the virus would grow, but there were hints that the exact methods we used were important: human cells were better than monkey cells; 33°C was better than 37°C; and synthetic medium 199 was better than the rest. And if we attempted further passes from culture to culture, volunteer tests were negative. The virus died out."
This is a great example of the illogical leaps that virologists make in order to disregard evidence that contradicted their presuppositions. If a cold failed to arise from the inoculation of cultured fluids, it wasn't due to the fact that there was no pathogenic "virus." It was that the "virus died out" resulting in the failure of the experiment.

The use of these more toxic cell cultured brews in order to generate the results that the researchers wanted to see was necessitated by the difficulty in establishing and distinguishing colds using only the nasal washings of sick patients. We can see evidence of this difficulty in establishing and distinguishing colds when looking at a 1958 paper from early in Tyrrell's tenure titled Transmission of the Common Cold to Volunteers Under Controlled Conditions. In the paper, it is said that over a 5 year period, the researchers observed more than 1,000 volunteers who were challenged with "infectious" nasal secretions obtained from persons with a common cold or with a blank solution used as a control. The nasal washings were not unadulterated as they were diluted with an isotonic salt solution buffered to pH 7.4 to which 0.5% yeast extract or 5% human Type O hemoglobin was added as a stabilizing protein. However, the researchers attempted to control the variables by also inoculating the control group with solutions containing 0.5% yeast extract or 5% human Type O hemoglobin. The volunteers were intranasally inoculated while in a supine position. Completely objective measures to determine the presence or absence of a cold were not available, so the researchers had to rely on subjective questionnaires filled out by the volunteers where a symptom score of 14 or more was established as the criterion for the presence of an experimental cold. However, this criterion failed to include those who subjectively developed a cold with fewer than 14 symptom points, which was a situation that occurred in nearly one-fourth of the experimental colds. It also included those who were said to develop symptoms from other causes. Thus, the researchers relied on the subjective analysis of a volunteer to determine if they had a cold, even though this was not considered entirely reliable, and included a measure where the presence of increased nasal discharge on three or more of the six days after the experimental challenge was required for those with a score lower than 14. This was meant to exclude those who were "over cooperative" volunteers who diagnosed themselves with a cold on the basis of a "few bizarre symptoms."
The researchers claimed that the experimental group would produce colds anywhere from 35-40% of the time. However, spontaneous colds also occurred in 10% of the control group. Both "infected" and "noninfected" volunteers would experience the main symptoms associated with the common cold such as headache, sneezing, chilliness, sore throat, malaise, nasal discharge, nasal obstruction, and cough. While it was said that the experimental illness caused more symptoms than the spontaneous colds observed among "noninfected" volunteers, the latter often did not have their full course of symptoms during the period of observation of 6 days. Moderate headache or headache and malaise were experienced by both groups, and it was chalked up to possibly being caused by the experiment rather than any "infection." Interestingly, experimental "infection" with common cold agents was almost never accompanied by fever, which is supposed to be the hallmark sign of a cold that distinguishes it from allergies. In fact, those said to be "infected" with colds had a significant displacement downwards in temperatures during the first three days after challenge. Thus, one must wonder if all that the researchers produced were simply allergic reactions to foreign proteins. Similar findings were presented by Dr. Andrewes in his 1950 paper, where in the experimental colds produced, "fever is rare. Malaise and headache at onset are common." Also of note was that the clinicians in this study examining both groups were unsuccessful in using nasopharyngeal signs in order to distinguish volunteers with a cold from those without one. The presence of certain bacterial strains was said to be strikingly similar among the "infected" and "noninfected" groups throughout the subsequent seven days without any increase in their prevalence.
While the researchers believed otherwise, they admitted that, even though they, and several other investigators, had succeeded in producing symptoms referable to the upper respiratory tract by the intranasal instillation of filtered nasal secretions, "the objection might be raised that these symptoms were merely reactions to the foreign material that was introduced." They also concluded that an experimental cold "cannot be readily detected by examination of the nose and throat even by a person well qualified in otolaryngology" as there is "great variation in the appearance of the nasopharyngeal mucosa among average well persons." Interestingly, in a seeming attempt to bolster their own results, the researchers cited various studies, along with their own unpublished data, stating that the nasal instillation of live "adenovirus" from a tissue culture harvest, live egg-passaged influenza "virus," bacteriophage, "noninfectious" nasal secretions, and several foreign chemicals did not cause symptoms after instillation into the nose, thus discrediting the supposed "infectiousness" of both "adenovirus" and "influenza" in the process. Despite the fact that within their study the control volunteers, who were given solutions said not to contain any "virus," also developed cold symptoms, the researchers ultimately concluded that the study was a success in showing that a "virus" can be transmitted by the nasal instillation of dilute, cell-free, nasal secretion from donors with a common cold.
Failure to Launch
The difficulty that the researchers under Tyrrell had in producing and/or distinguishing experimental colds was not much better during the early days of the CCU under Dr. Andrewes either. For example, Dr. Andrewes recounted in 1949 that, in an experiment using nasal washings from healthy patients that were tested on 28 other patients, 6 colds were produced. He admitted that there was no evidence that any "virus" was the cause of the colds. Thus, using nasal washings from healthy hosts with no "viruses" can result in the exact same symptoms seen in experimental groups using fluids presumed to contain a "virus."
In Dr. Andrewes' 1962 Harben Lecture, he recalled how they exposed normal volunteers to "infected" subjects who were at various stages of illness. However, he noted that: "To our surprise, very little cross-infection occurred." In fact, in the example provided, 19 people were "exposed" to those with colds for 10 hours, and only one person was said to be "cross-infected." The cold was claimed to be given to him by an "infected" person who had no symptoms of disease, i.e the asymptomatic excuse. Regardless, Dr. Andrewes noted that their findings lined up with those of Kerr and Lagen (1933-34) who also failed to obtain evidence of natural transmission of colds. Later attempts by the CCU were considered failures as well, as a second (0 out of 4) and third (1 out of 5) test with inoculated materials did not produce the expected results, as was the case with a "natural wild cold" which failed to pass on to any of the 5 healthy people exposed. As such, other avenues were searched for to try and demonstrate "cross-infections."
A later experiment led Dr. Andrewes to isolate a group of twelve volunteers all summer long on the uninhabited island Eilean nan Ron off the northern coast of Scotland. In mid-September, he sent a boat of "infected" volunteers to the island to interact with the previously isolated island group. According to Dr. Andrewes, the "infected" were "liberal in the way they disseminated nasal discharge on playing cards, books, cutlery, handles of cups, letters, chairs, door-handles, and tables" and they regularly coughed at the island group for hours from behind a blanket partition. Various methods were used in attempts to "infect" the islanders, and testing showed that fine droplets from the "infected" had travelled throughout the room. The "infected" even lived in a separate house for three days with some of the islanders, offering maximum exposure. However, none of the island group caught so much as a sniffle, even though considerable efforts were made to "infect" them. Dr. Andrewes recounted, "Much to our surprise no colds had developed in any of the 12 exposed 'islanders' by Sept. 29. It was particularly unexpected that none of party C caught colds, though very fully exposed." Dr. Andrewes got anxious and then sent a man who was said to have a "wild" cold to sit and interact with the island group for a while. Even though it was then claimed that three of eight eventually caught his "wild" cold, later demonstrations to "infect" the healthy through the air were considered unsuccessful.
The New York Times article pointed out other attempts where Dr. Andrewes would send volunteers off for long walks on cold days, turn off the heat in their flats, and even made them sit around in wet socks without any success in producing colds. He reflected, "We couldn't satisfy ourselves that chilling by itself did anything." In the article "The Sneeze Hunt" published in Leader magazine in April 1950, a quote from a volunteer was provided highlighting the lack of success:
"The eighth day – and all I can boast is a slight snuffle…something really must be done…The mist is heavy early next morning as, scantily-clad, I go down to the river…I plunge up to my knees in icy water, old shoes, socks, slacks and all…an hour later [I change] into dry clothes…We wait all day. Nothing happens…The irony of it."
Similar attempts to either induce or suppress the expression of cold symptoms in volunteers were made under Tyrrell's tenure as well, and these efforts were largely unsuccessful. This led Tyrrell to suggest that "perhaps we should leave the attack on the virus to the human immune system."
According to David Tyrrell's obituary write-up for Dr. Andrewes, when John Enders introduced his roller tube cultures of human embryo cells to propagate "poliovirus," these same techniques were implemented at the CCU under Dr. Andrewes watch. The researchers there acquired the nasal washings from a scientist who was doing much of the culture work for the CCU, and then inoculated the sample into plasma clot cultures of human embryo lung cells. Even though no cytopathogenic changes were observed, they serially passaged the culture and then inoculated volunteers who subsequently developed colds. The researchers assumed that a "virus" must have reproduced, and they reported the results in a paper published in the Lancet in 1953. After publication, however, Dr. Andrewes stated that "we could no longer repeat our own results," thus showing that the published results were erroneous and that the experiment was entirely unsuccessful.
Cold-Free Holiday
Regardless of whether the researchers attempted to "infect" the volunteers through the use of the unpurified nasal washings of those suffering common cold symptoms or with the toxic cell cultured creations devised under Tyrrell's watch, a main theme emerged amongst the populace concerning whether to take a chance on the common cold vacation. As noted by Professor Nigel Dimmock, who worked at the Common Cold Unit in the 1960s, "it was a good deal because the chances of getting a cold were pretty slim." The New York Times profile stated that most volunteers were relatively unruffled about the risks due to the fact that it was extremely hard, to the volunteers' delight and the staff's frustration, to "infect" another person with a cold even under the idealized conditions. According to Dr. Robert Philpotts, a staff virologist, "one of our biggest problems is giving people colds." He felt that if he could give 80 percent of the people colds, that they could have finished their work very quickly. However, the actual estimates varied between one in three (33%) and one in five (15%). Few of the volunteers caught colds, and they actually had largely pleasurable stays at the facility, with many people returning for multiple stays. There were several romances that blossomed, such as one that developed between a male guitarist and a female oboist who dueted together outside of their units. Reviews were almost entirely positive throughout its 4+ decade history. A male teacher, who was an early volunteer of the facility, recalled his two peaceful experiences there with neither visit producing a cold:
"It was a fine place. I was able to retreat in the monastic sense, once to read, the second time to revise for an impending examination. Everything was gently controlled and, although the Scottish matron was somewhat unnerving and terrifying, the lack of authority, apart from the very few things we were forbidden, was a good relaxation after a heavy term of teaching. And I was given a cold on neither visit."
Another teacher, a female who volunteered six times in eleven years, also had fond memories:
"Time flew, sewing, reading, going on the occasional walk. It was a complete break from the world, a time to return to the freedom of childhood without its restraints. The yellow trolley (bringing meals) was a highlight of the trials. Pavlov's dogs had nothing on us."
Ironically, Dr. Andrewes eldest son John was also a volunteer at the facility three times and stated: "Nobody succeeded in giving me a cold."


Even though it was admittedly very difficult to produce colds experimentally, Tyrrell noted that "many of the volunteers were quite eager to catch a cold, even to the point of imagining the symptoms." Evidence of this was seen in the 1958 study mentioned previously with the "over cooperative" subjects. Interestingly, it has been known since at least 1930 that volunteers could convince themselves that they had a cold if they believed that they were being "infected" with a cold producing agent. This was demonstrated by Alphonse Raymond Dochez in his paper Studies in the Common Cold. Oddly enough, this was the paper that convinced Dr. Andrewes that the common cold was due to a transmissable "virus" to the point where he adopted the views of Dr. Dochez as the CCU's working hypothesis. In the 1930 paper, Dr. Dochez not only noted that volunteers could convince themselves that they had a cold when they did not, he also stated that the filtrates, regardless of whether containing the assumed "virus" or not, caused stuffiness, sneezing, and headaches:
"It is very easy for an individual who is being used for a transmission experiment to believe that he has a mild cold although objective evidence is extremely slight or absent. Where, as in the beginning of our work, volunteers believed that we were trying to produce colds, they were self-convinced occasionally that they were suffering from a mild infection. This was much easier of belief as the filtrate in practically all the cases, negative and positive, causes some slight stuffiness of the nose, a little sneezing and occasionally slight headache."
As an example, Dr. Dochez spoke about a patient who was given an injection of sterile broth without "virus." When he was accidentally told by an assistant that he had failed to catch a cold, that night, the man began to suffer severe symptoms. When he was told the next morning that he had been misinformed about the nature of his injection, the man's symptoms disappeared within an hour:
"It was apparent very early that this individual was more or less unreliable and from the start it was possible to keep him in the dark regarding our procedure. He had inconspicuous symptoms after his test injection of sterile broth and no more striking results from the cold filtrate, until an assistant, on the second day after injection, inadvertently referred to his failure to contract a cold. That evening and night the subject reported severe symptomatology, including sneezing, cough, sore throat and stuffiness of the nose. The next morning he was told that he had been misinformed in regard to the nature of the filtrate and his symptoms subsided within the hour. It is important to note that there was an entire absence of objective pathological changes."
The power of the nocebo effect, which is where the belief that a negative outcome from a treatment or procedure actually causes the manifestation of that outcome and results in harm, is a well-known phenomenon. This was something acknowledged by researchers before, during, and after the CCU experiments. In the CCU's intake form, they advised that "the volunteer should not be bound to think that he will develop symptoms after being given nose drops." In fact, they admitted that "there is a good chance that he may not" as "some volunteers prove resistant to the virus inoculum anyway." They admitted that "by and large, only about one third of all volunteers actually develop symptoms." These symptoms are non-specific, and they are exactly the same as those attributed to hay fever and seasonal allergies. Thus, on top of the issues with patients manifestimg symptoms due to the belief that they may get a cold just from undergoing the experiment, the interpretation of a cold is entirely subjective which is why they utilized a double-blind set-up to try and mitigate "incorrect interpretations" by the researchers as well as to ensure that they did not imagine signs and symptoms that were not there. Just the action of injecting these solutions into the nasal cavities, regardless of whether they contain a "virus" or not, will result in symptoms such as headache, malaise, stuffiness, and sneezing, as noted by Dr. Dochez and the authors of the 1958 study. Thus, it can be easily concluded that it is due to the experimental procedure itself, along with the reaction, both physically and mentally, of the individual to the presence of foreign substances, that results in the occurrence of the non-specific symptoms which are then subjectively interpreted to be the common cold by the researchers based upon the inoculum given.
In order to actually conclude that they were successful in producing and studying cold "viruses," the researchers at the CCU had to go to great lengths to disregard evidence that showed otherwise:
- The inability to make numerous animals sick with the same disease.
- The inability to produce "coinfections."
- The inability to transmit "infections" through the air, even in heavily contaminated environments.
- The ability of the experimental procedure of intranasal inoculation itself producing fatigue, malaise, sneezing, and a stuffy nose.
- The great difficulty (15-33% "success" rate) to produce cold symptoms using "virus" samples as well as being unable to replicate the results consistently.
- The inability to come up with successful treatments and vaccines.
- The nocebo effect producing the same symptoms associated with the common cold.
- The control groups also coming down with the same symptoms of disease associated with the common cold despite being given solutions said not to contain any "virus."
While the textbooks may claim that the Common Cold Unit was successful in identifying common cold "viruses" along with transmitting and studying the disease, it is very clear looking at its history that it was anything but a success. For a facility that wanted to study the common cold "virus" by "infecting" their human guinea pigs, they had an awfully difficult time doing so resulting in an admittedly low "success" rate. The little "success" that they did have could easily be explained away by different confounding factors that were unrelated to the presence of any "virus." After various threats of closing the facility over its four decades in operation, the last trial was concluded in July of 1989, and the facility was finally closed for good in 1990. The Medical Research Council ultimately decided not to continue the work conducted at the facility anywhere else. Thus, the question must be asked: can a facility be considered successful in producing valuable research and evidence when it was closed down for "financial reasons" with its research halted completely? Closures do not happen if something is viewed as successful and worthy of investment. Giving out free all expenses paid vacations while paying staff and volunteers for their efforts with little results to show for it doesn't seem like a sound financial investment. Perhaps some interesting advice given to David Tyrrell by Dr. Andrewes was overheard by those with the pocket books who were looking for a return on their investments, and it made them realize that it was not meant to be:
"You shouldn't be interested in why volunteers given viruses get colds, but why so many don't!"
This article originally appeared on ViroLIEgy's Antiviral Substack.
29 Feb 2024 | 4:03 pm
ViroLIEgy 101: The Scientific Method
ViroLIEgy 101 is a series of articles meant to provide relatively short (by my standards) and concise explanations of key concepts regarding both germ "theory" and virology. I'm providing an overview on topics that are essential to the conversation that people may be confused with and have difficulty understanding, or areas that seem to be controversial when engaging in discussions with those defending the germ "theory" of disease.
Over the course of the last few years, others and I have been engaged in discussions with all kinds of people who defend germ "theory" and virology, from the everyday layman to actual scientists and virologists. One of the most stunning and alarming takeaways from many of these conversations is the outright confusion over the scientific method, a logic-based procedure that has characterized natural science since at least the 17th century and has been around for much longer. When it is brought up in these exchanges as a means to challenge the pseudoscientific (i.e. fake science) evidence presented by virologists, there is a decidedly mixed reaction. Some virologists and microbiologists, who agree that the scientific method exists while claiming that they adhere to it, demonstrate that they simply do not understand the scientific method, as was shown by plant virologist Thomas Baldwin, a.k.a. Sense Strand, in conversation as well as in the image he supplied below.

Some claim that there is no one method used by scientists, arguing that the steps that I regularly outline are my own creation or definition that I apparently pulled out of thin air. When challenged on this claim that the steps outlined are "my steps," they either have no answer (after outlining the exact same steps that I presented):

Or they end up inadvertently admitting that the steps that I presented are, in fact, the scientific method after previously claiming that they are not:



Even some who are on the "no virus" side do not believe in and outright deny the existence of the scientific method, claiming that it is a scam by doctors who "promote a made-up definition of science based on the so-called 'Scientific Method'" in order to con the public.

With so much confusion over what the scientific method is as well as whether or not it actually exists, I figured that it was as good a time as any to dive into the history of the establishment of the scientific method. What we will see is that these logical and rational steps not only exist as a method that was carefully molded over time into what they are today, but that these steps are crucial in determining what constitutes scientific knowledge. It will be clear why myself and others are confident in holding the evidence coming from virology (as well as other fields) to these standards. You will see that any evidence that was not derived from the scientific method is, by definition, pseudoscientific.
Defining Science and The Scientific Method
In order to properly discuss the scientific method, it is beneficial to define what exactly science is first. The word "science" actually stems from the Latin word scientia which translates to "knowledge." Ironically for virology, it is said that the original notion in the Latin verb was most likely "to separate one thing from another, to distinguish," which is something that virologists have a major problem doing, to the point where they literally changed the definition of "isolation." Regardless, while science may mean knowledge, knowing something in and of itself is not science. One can know that the sky is blue, but just knowing this fact does not constitute scientific knowledge. One can be an expert in all things related to Pokémon, but that does not mean that they are a scientist. In order for the knowledge to be considered scientific, it must meet certain criteria, as pointed out by The Science Council when they decided to define science in 2009. The Science Council is a UK organization established by Royal Charter in 2003, and their principal activity, according to their Wikipedia page, is "the promotion of the advancement and dissemination of knowledge of and education in science pure and applied, for the public benefit." According to their definition, science is defined as such:
"Science is the pursuit and application of knowledge and understanding of the natural and social world following a systematic methodology based on evidence."
The Science Council further elaborated on their definition by outlining what this systematic methodology that makes up science entails:
Scientific methodology includes the following:
- Objective observation: Measurement and data (possibly although not necessarily using mathematics as a tool)
- Evidence
- Experiment and/or observation as benchmarks for testing hypotheses
- Induction: reasoning to establish general rules or conclusions drawn from facts or examples
- Repetition
- Critical analysis
- Verification and testing: critical exposure to scrutiny, peer review and assessment
They highlighted observation, hypothesis testing, experimentation, analysis of results, drawing conclusions, and repetition along with verification as core components of the scientific methodology. The Science Council made an effort to explain exactly what the scientific methodology is that they are referring to, and used this as a central component of their definition of what science is supposed to be. However, The Science Council is not the only one to highlight the scientific method when defining science:
According to Merriam-Webster, science is defined as knowledge obtained through the scientific method:
knowledge or a system of knowledge covering general truths or the operation of general laws especially as obtained and tested through scientific method
Their definition of the scientific method involves observation, the formulation and testing of hypotheses, experimentation, and the collection of data:
principles and procedures for the systematic pursuit of knowledge involving the recognition and formulation of a problem, the collection of data through observation and experiment, and the formulation and testing of hypotheses
According to Vocabulary.com, science is defined as an empirical field that utilizes the scientific method to aquire knowledge:
"Science is an "empirical" field, that is, it develops a body of knowledge by observing things and performing experiments. The meticulous process of gathering and analyzing data is called the "scientific method," and we sometimes use science to describe the knowledge we already have."
Their definition of the scientific method includes observation, hypothesis testing, and experimentation, and within their further breakdown of the method, they state that scientists look to explain cause and effect relationships observed in nature:
"a systematic way of investigating to test a hypothesis"
"The scientific method is a process for experimentation that is used to explore observations and answer questions."
"Scientists use the scientific method to search for cause and effect relationships in nature"
From BiologyOnline.com, science is defined as a body of knowledge that is gained from the application of the scientific method:
A systematized body of knowledge in the form of hypotheses, theories, principles, models or laws that have been conclusively drawn from observed or verifiable facts or from experimental findings gained basically from the application of the scientific method.
Their definition of the scientific method involves investigating a phenomenon, the formulation and testing of a hypothesis, experimentation, gathering and analyzing data, and drawing conclusions:
A systematic approach to solving a problem by discovering knowledge, investigating a phenomenon, verifying and integrating previous knowledge. It follows a series of steps that evaluates the veracity or the feasibility of a prediction through research and experimentation from where the information obtained will be used as a basis in making conclusions.
The fundamental steps of scientific mA systematic approach to solving a problem by discovering knowledge, investigating a phenomenon, verifying and integrating previous knowledge. It follows a series of steps that evaluates the veracity or the feasibility of a prediction through research and experimentation from where the information obtained will be used as a basis in making conclusions.
The fundamental steps of scientific method are:
(1) Identifying the problem to solve
(2) Formulating a tentative answer or hypothesis
(3) Testing the hypothesis
(4) Gathering and analyzing data
(5) Making conclusions
Even Wikipedia understands that science requires the use of the scientific method:
Scientific research involves using the scientific method, which seeks to objectively explain the events of nature in a reproducible way.[167]
The Wikipedia scientific method page lays out observation, creation of a hypothesis, testing through experimentation, and analyzing the results in order to accept or reject the hypothesis. They go so far as to say that these are a definitive series of steps for all scientific enterprises:
The scientific method involves careful observation coupled with rigorous scepticism, because cognitive assumptions can distort the interpretation of the observation. Scientific inquiry includes creating a hypothesis through inductive reasoning, testing it through experiments and statistical analysis, and adjusting or discarding the hypothesis based on the results.
The above mentioned are principles of the scientific method, a definitive series of steps applicable to all scientific enterprises.
Wikipedia even supplied a nifty little graphic demonstrating the scientific method.

Finally, according to Black's Law Dictionary, considered America's most trusted law dictionary and one of the most valuable reference tools to the legal community, the legal definition of science is knowledge that is gained through the application of a scientific method:
Knowledge that is comprised of verifiable and measurable facts that have been acquired by the application of a scientific method.
The legal definition of the scientific method is a step-by-step approach that involves identifying and defining a problem, hypothesis formation, testing the hypothesis through experimentation, gathering and interpreting the data, and repeating the process:
A step-by-step approach to solving problems. Identify and define the problem, accumulate data, formulate a hypothesis, conduct experiments to prove hypothesis, interpret results in an objective manner and repeat.
As can be seen, the scientific method is a core component of what makes up scientific knowledge. You can't have one without the other. The steps outlined in the above definitions line up exactly with what myself and others have highlighted in our conversations with those who deny the method.

The steps of the scientific method are clearly not our own creation. They are not a scam or a con used to deceive the public. Nature.com even shared the exact same steps when defining science and stated that "Any field of study which adheres to this process is considered science," and that by using the scientific method, "a proper characterization and by extension, definition, of science can be made." Thus, it can easily be said that without adhering to these steps and gaining evidence using this methodology, the knowledge aquired is not scientific.
The History of The Scientific Method
Now that we have a definition for what constitutes scientific knowledge and we can see that adherence to the scientific method is essential to aquiring this knowledge, this leaves us with the question as to where exactly these steps that make up the scientific method actually came from. Let's take a brief look at the documented history to find out exactly how this methodology was established.
According to the 2019 paper Perspective: Dimensions of the scientific method by clinical professor of biological science and researcher Eberhard O. Voit, the roots of the scientific method stretch all of the way back to ancient Greece with the work of Aristotle and Herophilus in the 3rd century. Aristotle was considered the first to define and conduct empirical studies with concrete evidence, purpose, and logic. This framework of empirical study based on logic and reason established by the Greeks was expanded upon by the Arabs with the work of Avicenna and Alhazen (also known as al-Haytham) around 1,000 AD, who developed meticulous methods of experimentation utilizing "controlled scientific testing in order to verify theoretical hypotheses and substantiate inductive conjectures." The English philosophers Robert Grosseteste and Roger Bacon contributed to the expansion of the scientific method in the Middle Ages around 1200-1250 AD by promoting "the conception of science as the inductive study of nature, based on and tested by experiment." However, according to many researchers, the scientific method, as we know it today, was crystallized around the 17th and 18th century with the work of English philosopher and statesman Sir Francis Bacon and French philosopher and scientist Rene Descartes, both of whom strove for objectivity based upon observations rather than preconceived ideas and superstitions:
"This scientific method has deep roots going back to Aristotle and Herophilus (approximately 300 BC), Avicenna and Alhazen (approximately 1,000 AD), Grosseteste and Robert Bacon (approximately 1,250 AD), and many others, but solidified and crystallized into the gold standard of quality research during the 17th and 18th centuries [1–7]. In particular, Sir Francis Bacon (1561–1626) and René Descartes (1596–1650) are often considered the founders of the scientific method, because they insisted on careful, systematic observations of high quality, rather than metaphysical speculations that were en vogue among the scholars of the time [1, 8]. In contrast to their peers, they strove for objectivity and insisted that observations, rather than an investigator's preconceived ideas or superstitions, should be the basis for formulating a research idea [7, 9]."

Even though many credit Aristotle with setting the foundation for the empirical scientific method while recognizing Francis Bacon and Rene Descartes for solidifying it, the work of the Arab scientists, particularly Ibn al-Haytham, is where the steps that resemble the modern version of the scientific method were first established. Al-Haytham was known for being a mathematician and astronomer who made significant advances in the field of optics. He is considered the architect of the scientific method due to his detailed writings of his own procedures, focusing on the importance of observation and experimentation. In the paper Al-Haytham the man of experience. First steps in the science of vision, author Rosanna Gorini stated that the majority of the historians consider al-Haytham as the one who pioneered the modern scientific method. With his writings, al-Haytham established experiments as the standard of proof in the field as his investigations were based on evidence obtained through experimentation rather than on abstract theories. He wanted to ensure that his experiments were systematic and repeatable. The steps attributed to al-Haytham's method include:
- Observation of the natural world
- Stating a definite problem
- Formulating a robust hypothesis
- Test the hypothesis through experimentation
- Assess and analyze the results
- Interpret the data and draw conclusions
- Publish the findings
As can be seen, the core concepts that make up what we know of as the scientific method today were being utilized by al-Haytham around 1,000 AD. Due to the excellence of his scientific method utilized some 500 years before the "Scientific Revolution," al-Haytham has become known as "the first scientist" by some historians, with his great influence on science extending well beyond the Arab world. Roger Bacon, who was one of the earliest European proponents of the scientific method, was inspired by the writings of al-Haytham in his own work about 200 years later. Bacon wanted to confirm the findings of Aristotle, whose work he was teaching to his students at the time. By utilizing the methods of al-Haytham, whom Bacon knew about thoroughly to the point where he intended his Perspectiva (part V of his Opus Maius) to be an interpretation of al-Haytham's theory, Bacon discovered that many of the Greek philosopher Aristotle's findings were actually incorrect. His version of al-Haytham's scientific method involved four crucial steps:
- Observation
- Hypothesis
- Experiment
- Verification
The work produced by Roger Bacon earned him the nickname of "Britain's first scientist," and there is evidence that he strongly influenced Sir Francis Bacon (not related) a few hundred years later when the scientific method was said to be codified during the "Scientific Revolution" of the 17th and 18th centuries. Francis Bacon contributed to solidifying the scientific method within the field by emphasizing and promoting the inductive process, relying on both observation and experimentation to form a conclusion. His method utilized experiments to manipulate nature in order to attempt to prove the hypotheses wrong. As an example, Francis Bacon argued that, in order to prove that disease developed due to external causes, healthy people needed to be exposed to the variables individually so that it could be determined if any of them were a potential cause. He insisted that this must be confirmed through repeated experimentation. We know that this is an area that has regularly refuted virology:
"For example, in order to test the idea that sickness came from external causes, Bacon argued that scientists should expose healthy people to outside influences such as coldness, wetness, or other sick people to discover if any of these external variables resulted in more people getting sick. Knowing that many different causes for sickness might be missed by humans who are unable or unwilling to perceive them, Bacon insisted that experiments must be consistently repeated before truth can be known: a scientist must show that patients exposed to a specific variable more frequently got sick again, and again, and again."
Francis Bacon and the Scientific Revolution

Eberhard Voit noted that the traditional scientific method was further established throughout this period by the work of researchers such as Rene Descartes (importance of deduction), Sir Isaac Newton (incorporated both induction and deduction), Karl Popper (the concept of falsifiability), and many others, and that their work throughout the centuries cemented the scientific method into what it is today; a method that is ultimately based upon formulating and testing hypotheses from observations. From the results of these tests, a deduction is made regarding whether the hypothesis is presumably true or false. Voit pointed out that, while it is often presented in discrete steps, the scientific method should be seen as a form of critical thinking that is subject to review and independent validation. The scientific method is very influential and has proven valuable in prescribing valid experimentation and affecting the way we attempt to understand nature. He stated that the scientific method has become "deeply ingrained in the scientific psyche, and it is now taught as early as middle school in order to teach students valid means of discovery." Even though various researchers influenced the method along the way, the "conceptual scaffold remained essentially unchanged." This method has since guided research studies, fundamentally influencing the thoughts on the process of scientific discovery to the point that nonadherence to the scientific method is seen as "lacking in rigor," leading to irreproducible and irreplicable results.
Breaking Down The Scientific Method
Now that we have established the core steps of the scientific method, let's examine them in more detail. In the Blinded by Pseudoscience article that I wrote a year ago, I went through the main steps of the scientific method and provided descriptions for each that I am sharing here. The article goes into more detail on how virology is unable to adhere to the scientific method and how it is, in fact, pseudoscience, so I recommend checking it out for further details.
1. Observe a Natural PhenomenonThis may be the most controversial of the core steps as people try to argue over what is considered a phenomenon. However, there should be no confusion when we define the word as it is most commonly understood; a phenomenon is an observable fact or event. A natural phenomenon is an observable fact or event that occurs in nature that is not man-made nor influenced or manufactured by human engineering or intervention. The cause or explanation of this observation is in question which leads one to start to investigate the matter scientifically in order to provide an explanation. Observing a natural phenomenon is usually done through the senses either by sight, sound, taste, touch, and smell. However, some phenomena are unable to be detected directly through the senses and require enhancement through the aid of technology such as microscopes, telescopes, stethoscopes, etc. Some examples of natural phenomena which are not man-made include lightning/thunder, volcanic eruptions, weather, decomposition, earthquakes, fire, etc. It is through the observation of the phenomenon that the necessary questions are asked in order to move into the next step in the process, forming a hypothesis.
2. Alternative HypothesisThe hypothesis is the foundation of the scientific method. It is an educated guess as to a possible explanation for what has caused the observed phenomenon. In order to have a valid hypothesis, there are two crucial elements that must be defined from the very start. These are the independent and dependent variables. The independent variable (IV) is the presumed cause of the effect that was observed. The IV must actually exist and be able to be varied and manipulated throughout experimentation to see what affects it may have, if any. It cannot be the end-result of the experiment. The dependent variable (DV), on the other hand, is the effect that was observed and that the researcher is looking to identify the root cause for. Unlike the IV, the DV cannot be directly manipulated as it is entirely dependent upon the manipulation of the IV.
Once both variables are identified, a hypothesis can be formulated. This is written as an if-then statement and drawn up as a possible explanation as to what may happen to be discovered upon experimentation. An example would look like this:
"If I water my plant every day, then it will grow."
In this example, the water is the IV while the growth rate of the plant is the DV. Along with these variables, there are other factors that must be identified as well, known as control variables. These are the factors that may influence the outcome of the experiment. In our example, these could include the amount of sunlight, the type of soil, the time of day, the temperature, the weather, indoor or outdoor environment, etc. Control variables must be accounted for and must remain unchanged throughout the course of the experiment. This is to ensure that any effect attributed to the IV was actually a result of the IV alone and not due to other confounding factors.
 3. Null Hypothesis
3. Null Hypothesis
An absolutely essential component of the hypothesis is that it must be falsifiable, meaning that it can be proven wrong. This is why one must also be able to establish a null hypothesis, which assumes that there is no relationship between the IV and DV. In other words, it is the exact opposite of the alternate hypothesis. Using our earlier example, it would be written simply as such:
"If I water my plant every day, it will not grow (or it may grow less or may die)."
It is this very concept of falsifiability that is a hallmark of true science. If one is repeatedly unable to falsify the alternate hypothesis, this is a very strong indicator that the results are indeed valid scientifically.
4. Test/ExperimentIt is at this stage where the real heart of science takes place. In order for the knowledge gained to be considered scientific, the hypothesis must be testable through experimentation. This is where the hypothesis will either be proven or disproven in regard to the causal relationship between the IV and the DV. The experiment must focus on only changing one variable at a time and must be repeated numerous times. The main experiment will coincide with control experiments to ensure that the hypothesized results are only seen with the experimental group. In order to be considered a success, the expected results must not be seen in the control group and must be reproduced more than once.
Going back to our water and plant example, we could plant seeds in two identical pots with the same soil. We would need to figure out how much water we want to use and then water our experimental pot daily while our control pot receives water once a week. As the plants grow, the height of each plant would be measured to see if the amount of water had any effect on the growth of the plant.
5. Analyze the Observation/DataAfter experimenting, the data is collected and ready for analysis in order to confirm or reject the hypothesis. This is rather self-explanatory. In our plant scenario, the heights would be measured to see what kind of difference may have been noticed. Did the experimental plant grow faster? Or perhaps daily watering resulted in over-watering and the death of the plant. How did the results compare with the control? Which plant fared better overall? Once completed, the experiments can be run again, if validated, in order to see if the results are repeatable and reproducible.
6. Validate/Invalidate HypothesisThis is another self-explanatory step. Either the experiment produced the intended result, thus confirming the alternative hypothesis, or it did not, thus confirming the null hypothesis. If it did not confirm the alternative hypothesis, then it is back to the drawing board to either come up with a new hypothesis and/or examine the variables which may have impacted the experimental results.
There Is No Science Without The Scientific Method
"Scientific knowledge can only advance when all scientists systematically use the same process to discover and disseminate new information. The advantage of all scientific research using the Scientific Method is that the experiments are repeatable by anyone, anywhere."
https://extension.unr.edu/publication.aspx?PubID=4239
The image above is from the U.S. National Science Foundation (NSF) which was established by Congress in 1950 as "an independent federal agency that supports science and engineering in all 50 states and U.S. territories." In the document that the image is obtained from, the NSF states that the scientific method is "a series of steps that a scientist follows to analyze and answer a question about a specific observation." As can be seen, the steps that are listed include observation, the formulation of a hypothesis, testing through experimentation, examining the data, and forming a conclusion. The National Institute of Environmental Health Sciences, a part of the NIH, states that "a good scientist learns about the world by using the scientific method" and that "all fields of science use the scientific method as a framework to make observations, gather data, and draw conclusions." It goes on to lay out the steps of the scientific method such as forming a hypothesis, testing it through experimentation, analyzing the results, and reporting conclusions. The National Institute for Standards and Technology (NIST), another governmental agency, states that the scientific method is the "systematic pursuit of knowledge involving the recognition and definition of a problem; the collection of data through observation and experimentation; analysis of the data; the formulation, evaluation and testing of hypotheses; and, where possible, the selection of a final hypothesis." We can find many other sources (examples here, here, here, and here) that all list the same steps as the NSF, the NIH, and the NIST as these steps are the core of scientific method, and they allow one to logically and rigorously test hypotheses in an unbiased fashion in order to obtain scientific knowledge. Without adherence to the steps of the scientific method, and without the ability to establish a falsifiable hypothesis based upon observed natural phenomenon that is capable of being tested experimentally, the evidence and knowledge gained are considered to be pseudoscience by definition.
According to Oxford Languages, pseudoscience is defined as such:
a collection of beliefs or practices mistakenly regarded as being based on scientific method.
According to BiologyOnline.com:
Any body of knowledge, methodology, belief, or practice purported to be scientific but which fails to comply with the scientific method, lacks supporting evidence, or cannot be tested in practice or in principle.
According to TechTarget.com:
Pseudoscience is a proposition, a finding or a system of explanation that is presented as science but that lacks the essential rigor of the scientific method.
According to Study.com:
Pseudosciences often appear to be a genuine science, but they do not follow the scientific method.
And once again, even Wikipedia understands that without the scientific method, it isn't science:
Pseudoscience consists of statements, beliefs, or practices that claim to be both scientific and factual but are incompatible with the scientific method.
As scientific knowledge must be aquired through the adherence to the steps of the scientific method, perhaps this is why many scientists and virologists try so hard to deny the scientific method, even to the point of claiming that it doesn't exist or that it is a scam used to con the public. Perhaps they realize that the steps actually conflict with the results of their own work and beliefs. Perhaps, upon realizing that the scientific method does exist, they come to the understanding that the work that they produced may not be scientific at all, and that, instead of practicing science, they have been engaged in pseudoscience all along. Perhaps, upon this realization, they go up against their own cognitive dissonance, which frightens and angers them.
Had these scientists and virologists understood and adhered to the scientific method, we wouldn't have a situation where most published scientific research findings are false, and we wouldn't be stuck in a reproducibility and replication crisis with no end in sight. Had the scientific method been followed, the repeatedly disproven and falsified germ hypothesis would have never been elevated to a "scientific theory," and the entire field of virology would have remained within the realm of fantasy and pure imagination right where it belongs. Instead, we find ourselves in a world that has largely misplaced and disregarded its method for determining true scientific knowledge, which has led to the mistaken belief that pseudoscience is science, and a generation of scientists and virologists, along with the laymen who listen to them, that can't tell the difference.
This article originally appeared on ViroLIEgy's Antiviral Substack.
27 Feb 2024 | 2:59 pm
The Final Pandemic
I imagine that anyone who follows my work is most likely already familiar with the dynamic duo of Drs. Sam and Mark Bailey. Since 2020, this brilliant pair have been at the forefront of exposing the fraud of germ "theory" and virology, putting out numerous entertaining and truly enlightening videos illuminating various aspects of the pathogenic lie. Along with her excellent video content, Dr. Sam Bailey helped to co-author the 3rd edition of the amazing book Virus Mania with Torsten Engelbrecht, Dr. Claus Kohlein and Dr. Stefano Scoglio. Meanwhile, Dr. Mark Bailey put out two powerful essays striking at the heart of the scam with The COVID-19 Fraud & War On Humanity and A Farewell to Virology. The Baileys also took on the task of bringing Dr. Ulrich Williams' material to a whole new audience with their updated re-release of his work in the book Terrain Therapy: How To Achieve Perfect Health Through Diet, Living Habits & Divine Thinking.
Never ones to take a moment to rest, the Baileys have struck again with their latest masterpiece in The Final Pandemic – An Antidote to Medical Tyranny. This book carries all of the hallmarks of the meticulous and exhaustive research we have come to love and expect from the Baileys. They utilize their wonderful skills to shed even further light on the problems with the germ "theory" and allopathic model. I am in awe of how deftly they are able to present the information, like two talented virtuoso's at the top of their profession, working harmoniously together to bring light to a whole new audience. I am extremely excited for everyone to experience this book!
Our new book The Final Pandemic – An Antidote to Medical Tyranny has been over 18 months in the making and we are pleased to announce that it is now available in e-book, paperback and hardcover versions. The idea for this book arose from Professor Timothy Noakes, MD, the renowned nutrition and sports scientist who was a welcome signatory to the 'Settling the Virus Debate' Statement in 2022. After reading Virus Mania in 2021, Tim became a virus sceptic and suggested the need for a high-impact punchy book with the aim of reaching an even wider audience.
The book is now reality at around 55,000 words, or around 240 pages in the hardcopy versions, with well over 400 references. If you have struggled to get friends and family members to look at this paradigm-changing material then this may be your best chance yet. And for our seasoned audience there is plenty of thought-provoking and never seen before content regarding virology, germ theory and allopathic medical mayhem.
Following thousands of hours of research and development, The Final Pandemic – An Antidote to Medical Tyranny is structured as follows:
Acknowledgements
Foreword by Prof. Tim Noakes
Prologue
Introduction
Chapter 1 – Creating a Pandemic
Allopathic Medicine Invents Diseases
COVID-19: The Bait-and-Switch
Meaningless Cases
Enter "Patient Zero"
Clustering and "Asymptomatic Transmission"
'Typhoid Mary' – The Original "Superspreader" Story
Death of "Whistleblower" Doctors
Prepare the Public with Hollywood Blockbusters
Chapter 2 – Scapegoats for Disease
Invent a Disease and Blame it on Animals
Blame SARS on Bats with no Evidence
Slaughter Millions of Animals to Drive the Fear
Blame the Pox on Gay Men (and Animals Again)
Suggest the Disease came from a Lab (and Animals Again)
The Washington Post Connects no Dots
Fear-inducing "Viruses" Like Ebola…that Never Arrive
Chapter 3 – The History of Misplaced Beliefs
What Human-to-Human Transmission?
But Can't You Catch a Cold?
Blaming Nutritional Deficiencies on Germs
Blaming More Dietary Problems on Germs
Blaming the Effects of Environmental Toxins on Germs
"Treatments" that Cause the Disease?
Don't Worry if the Germ Even Exists
Death-dealing Drugs Marketed as "Life-saving"
Chapter 4 – Pandemics of Testing
PCR Already Known to Cause False Pandemics
The PCR Exposed Whooping Cough's Faulty Science
What is the Polymerase Chain Reaction?
Why was SARS-2 (COVID-19) Bigger than SARS-1?
How to Create "Virus Genomes"
Chapter 5 – Press Release Science
Programming the Public
Celebrity Cases
Rigging the Playing Field
"Stuffing Their Mouths with Gold"
Persecution of Those Questioning the Narrative
Case Study: The Suppression of The Perth Group
Chapter 6 – All Pandemics Lead to Vaccines
What are Vaccines Doing?
The Bill Gates Factor
Big Pharma Invents Demand
Case Study: 'HPH' & Her Licence to Lie
The Cause of the Rise in Vaccine "Misinformation"
Summary
Epilogue
About the Authors

The Baileys also produced a nice video announcing the arrival of the book:
https://drsambailey.substack.com/p/the-final-pandemic
Please help support the Baileys efforts, enjoy the amazing fruit of their labor, and pass this book on to those who need it the most. It is yet another exciting way to present the message to those who need to hear (and read) it.
16 Feb 2024 | 3:20 pm
Measles Magic
If you have been paying attention to recent headlines here in the US, you will notice that it is time once again for the measles magic show. In other words, it is time for virologists to pull the measles "virus" out of their hats so that it can rear its head in order to frighten the ignorant into allowing toxic injections into themselves and their children. While measles cases are said to occur in the US every year, the alarm bells rung by the CDC and within the mainstream media happens every so often when there needs to be a clamp down on anti-vaccine messaging as well as a push to increase vaccination rates. Remember the scary headlines alerting the people to a measles outbreak in Disneyland in 2014? It was the perfect set-up to strike down nonmedical vaccine exemptions that were increasing in California and elsewhere. The media focused on a "spread" through the unvaccinated population and highlighted vaccine hesitancy as a primary driver of the outbreak. This led to a "positive" outlook and support for vaccination.
Revisiting the 2014-15 Disneyland measles outbreak and its influence on pediatric vaccinations"The outbreak capped a year with the highest number of measles cases reported in two decades and came amidst increasing trends in nonmedical vaccine exemptions in California and elsewhere. Because of its sensational story line and spread among unvaccinated populations, the outbreak received a high level of media coverage that focused on vaccine hesitancy as a primary driver of the outbreak. This media coverage and the ostensible public support for vaccines that followed led some to hypothesize that the outbreak might have a "Disneyland effect," or a positive influence on the uptake of pediatric measles vaccine."
https://pubmed.ncbi.nlm.nih.gov/34495822/

However, the Disneyland Measles Massacre wasn't even the "main" measles "outbreak" in 2014. That distinction belongs to the Amish in Ohio where an "outbreak" was blamed on an Amish missionary who traveled to the Philippines. In the end, there were 382 Amish said to be "infected" with the measles "virus." Not a single person died. Regardless, the missionary, who was originally diagnosed with dengue, was given the blame for being unvaccinated and bringing the measles "virus" back to spread amongst the unvaccinated. While this "outbreak" helped to clamp down on anti-vaccination sentiment riled up by Jenny McCarthy that year, it was the perfect vehicle to convince the masses that it is unvaccinated travelers bringing back diseases in from other countries. This is a theme that the CDC has utilized time and time again:
How an Amish missionary caused 2014's massive measles outbreak"Last year was terrible for measles in the United States: there were 644 cases — the highest annual caseload in two decades. Granola-crunching Californians, wealthy Oregonians, and Jenny McCarthy anti-vaccine acolytes have taken much of the blame for this spike. The Washington Post even pointed to Orange County — the location of the current Disneyland outbreak — as "Ground Zero in our current epidemic of anti-vaccine hysteria."
But that's wrong. The real story behind the 2014 outbreak isn't on the West Coast. It's in Ohio Amish country, where a missionary returning from the Philippines turned an otherwise unremarkable year for this virus into one of the worst in recent history."
"The outbreak that Fletcher spent months working to contain ultimately infected 382 Amish Ohioans by the time it was declared over in August of last year. Nobody died, but nine wound up in the hospital with more serious symptoms."
"But in the first half of 2014 alone, there were 288 cases. And nearly all of them, the CDC researchers wrote in findings published last June, stemmed from Americans traveling abroad and returning with the disease.
"Of the 288 cases, 280 (97 percent) were associated with importations from at least 18 countries," they wrote. Many of these travelers were coming back from the Philippines, which has been dealing with a massive outbreak since fall 2013.
"What we've seen — since the epidemic of measles was interrupted in 2000 — is that we are continually getting measles coming in from overseas," says Jane Seward, deputy director of the viral diseases division at the CDC. "More often than not, it's US residents who go overseas for a trip — to say, Europe, where they don't think they need to be vaccinated. They bring measles back."
"In the Ohio case, "patient zero" had traveled to the Philippines on a missionary trip. (In case you were wondering, he took a plane. Miller explained, "Some Amish fly. Some don't.") At the time, the Philippines happened to be facing a massive measles outbreak, with tens of thousands of cases.
When he returned to Ohio, and fell ill, a doctor misdiagnosed him with Dengue fever, so he continued to pass his disease along to friends and neighbors, many of whom had refused the vaccine out of those concerns over adverse effects.
Fletcher describes it as a "perfect storm:" an unimmunized traveler going to a place with an outbreak and bringing an infectious disease back to an unprotected community."
https://www.vox.com/2015/1/29/7929791/measles-outbreak-2014
The scare tactics worked to convince some within the notoriously anti-vaccination Amish community to get at least one dose of the MMR vaccine:
Vaccination of Amish limited 2014 Ohio measles outbreak"In response to the outbreak, which occurred between March 24 and July 23, 2014, some 10,644 members in a community of 32,630 Amish in the Ohio settlement received at least one dose of the MMR vaccine, with 1,585 getting two doses."
In 2017, there was a growing concern that the Somali community in Minnesota was influenced by anti-vaccine information. The child vaccination rates for measles, mumps, and rubella (MMR) had plummeted from 92% in 2004 to 42% in 2014 amid fears that Somali children have unusually high rates of autism. Thus, a measles "outbreak" was declared that suspiciously affected primarily unvaccinated Somali children.
"In 2017, 75 measles cases were reported as a result of an outbreak that began in Hennepin County involving the Somali community. This was the largest measles outbreak experienced since 1990, and the second major measles outbreak to affect the Minnesota Somali community in 6 years."
https://www.health.state.mn.us/diseases/reportable/dcn/sum17/measles.html
Fortunately for the fear promoters, the scare tactics worked again, and the vaccination push increased rates amongst the Somali American children from 30 a week in March to 500 in May.
"But the measles outbreak was shifting perceptions at last, she said. Weekly MMR vaccination rates among Somali American children have climbed from 30 or 40 a week in March to about 500 a week in May."
https://www.bmj.com/content/357/bmj.j2378.long
In 2019, there was a measles "outbreak" in New York City said to have started due to an unvaccinated child who returned home from Israel with measles symptoms. The Orthodox Jewish Community was singled out for their lack of a belief in vaccination as well as their concerns over the dangers of the toxic injections. Thus, a targeted vaccination promotion campaign ensued to combat this growing awareness.
Consequences of Undervaccination — Measles Outbreak, New York City, 2018–2019"During focus groups conducted by the Department of Health and Mental Hygiene after a mumps outbreak in 2009–201023 in this same community, mothers expressed concern about vaccines and autism, vaccine safety, and whether children are receiving too many vaccines too early in life. Antivaccination sentiments were deepened when an organization targeted this community with misleading materials regarding the risk of vaccination.19 To address these concerns, the Department of Health and Mental Hygiene reprinted and mailed two booklets that provided accurate information about vaccines to 29,000 households in Borough Park and Williamsburg, and a campaign was launched to combat vaccine myths in affected communities.24,25"
https://www.nejm.org/doi/full/10.1056/NEJMoa1912514
The threat of a measles "outbreak" and the vaccination propaganda efforts led to an increase in the percentage of children in Williamsburg who received at least one dose of MMR vaccine, rising from 79.5% to 91.1% among children 12 to 59 months of age. Thus, the scare tactics were once again successful in nudging the sheep in the direction that the pharmaceutical overlords wanted them steered in.
Even though the US officially declared that measles was successfully eliminated (considered an absence of continuous disease transmission for greater than 12 months) from the country in the year 2000, pocket outbreaks tend to conveniently pop up just when there is a growing chorus of anti-vaccination sentiment emerging as well as noticeable decreases in overall vaccination coverage. This is the case now as, due to the declining vaccination rates brought about by the "pandemic" and the distrust in the mRNA vaccines, the "threat" of new measle "outbreaks" in the unvaccinated is being used to try and instill the necessary fear to drive vaccination rates up to where the pharmaceutical interests want them to be. However, with measles eliminated from the US over 20 years ago, how are they able to drum up these measles "outbreaks" right at the most opportune moments in order to propagandize the populace? How are they able to make it look as if the unvaccinated are the main contributors of these "outbreaks?" Let's have a look at a few of the tricks that they have up their sleeves and see if we can take the mysticism out of their magic.

The first part of the trick to increase measles cases is rather easy to spot. The CDC simply sends out an alert to healthcare workers to be on the lookout for any cases of disease that may meet the clinical criteria as a measles case. Prior to any alerts, healthcare workers do not regularly look to measles as a diagnosis if they come across measles-like disease as it is not considered an endemic (a disease that is always present in a population within a geographic area, typically year-round) disease in the US. In the alert, the CDC highlights specific groups who healthcare workers are to be on the lookout for, which is anyone who is linked to international travel as well as anyone who is unvaccinated or partially vaccinated that can be linked to them. However, if a person meets the necessary measles case definition and requirements, but they either had measles in the past or have had their measles vaccines, the CDC assumes that these people are "protected" from the disease and are not measles cases:
CDC warns health care workers to be on alert for measles amid rising number of cases"The Centers for Disease Control and Prevention (CDC) is warning clinicians to remain on alert for measles cases due to a growing number of infections.
Between Dec. 1, 2023, and Jan. 23, 2024, there have been 23 confirmed cases of measles including seven cases from international travelers and two outbreaks with five or more infections each, according to an email sent this week."
"According to the CDC, most measles cases in the U.S. occur when unvaccinated or partially vaccinated Americans travel internationally, contract the disease and then spread it to those who are unvaccinated upon their return."
"The CDC says anybody who either had measles at some point in their life or who has received two doses of the MMR (measles, mumps, rubella) vaccine is protected against measles."
https://www.yahoo.com/gma/cdc-warns-health-care-workers-220221620.html
From the alert sent out by the CDC, international travel is noted as a condition for suspicion, and it is claimed that most cases are amongst the unvaccinated. Healthcare workers are told to look for anyone presenting with febrile rash and symptoms consistent with measles, which are nonspecific, such as cough, coryza, or conjunctivitis. However, it seems that they are only to look to measles as a possible diagnosis if the ill patient traveled abroad, especially to places where measles "outbreaks" are ongoing.
Stay Alert for Measles Cases"Between December 1, 2023 and January 23, 2024, the Centers for Disease Control and Prevention (CDC) was notified of 23 confirmed U.S. cases of measles, including seven direct importations of measles by international travelers and two outbreaks with more than five cases each. Most of these cases were among children and adolescents who had not received a measles-containing vaccine (MMR or MMRV), even if age eligible.
Due to the recent cases, healthcare providers should be on alert for patients who have: (1) febrile rash illness and symptoms consistent with measles (e.g., cough, coryza, or conjunctivitis), and (2) have recently traveled abroad, especially to countries with ongoing measles outbreaks. Infected people are contagious from 4 days before the rash starts through 4 days afterwards.
Measles cases often originate from unvaccinated or undervaccinated U.S. residents who travel internationally and then transmit the disease to people who are not vaccinated against measles. The increased number of measles importations seen in recent weeks is reflective of a rise in global measles cases and a growing global threat from the disease."
https://emergency.cdc.gov/newsletters/coca/2024/012524.html
Why does the CDC need to alert healthcare workers to be on the lookout for very specific parameters (such as travel history, vaccination status, certain nonspecific symptoms) in order to look for measles as a potential diagnosis in someone suffering measles-like disease? Shouldn't the healthcare provider be able to look at a measles case and be able to tell what it is in order to diagnose it? If you thought that was the case, you'd be wrong. According to Amesh Adalja, MD, an assistant professor who specializes in "infectious" diseases at the Johns Hopkins Center for Health Security in Baltimore, doctors may suspect measles if there is a history of not being vaccinated that accompanies the nonspecific symptoms of disease, but this suspicion must be "confirmed" with a laboratory test. Even then, some doctors won't suspect measles as they have no idea what a measles case even looks like:
"In general, if a doctor is examining a child with a fever, rash, runny nose and red eyes, and usually some history of not being vaccinated, they will suspect measles," says Dr. Adalja. A laboratory test that uses a nasal or oral swab can confirm the diagnosis, he adds.
The diagnosis may not always be as straightforward as it sounds, says Adalja. "In the United States, many doctors have never seen a case of measles, and so sometimes they don't even think to suspect it," he says."
https://www.everydayhealth.com/measles/guide/
Dr. Adalja's statement that most healthcare workers have never seen measles and that laboratory confirmation is required in order to make a diagnosis is backed up by the Minnesota Department of Health which stated the same:
"Many U.S. health care providers have never seen a case of measles. Without proper laboratory testing, measles cannot be diagnosed."
The MN Department of Health reiterated that a clinical diagnosis must be confirmed with laboratory testing in another document as well, meaning that clinical diagnosis alone is unreliable:
"A clinical diagnosis of suspect measles must be confirmed with laboratory testing."
The Washington State Department of Health agreed, saying that clinical diagnosis is unreliable and must be laboratory confirmed:
"Clinical diagnosis is unreliable, therefore cases must be laboratory confirmed."
The National Institute for Health and Care Excellence in the UK also agreed by stating that clinical diagnosis is unreliable and must be "confirmed" via laboratory results:
"Measles is a notifiable disease. Clinical diagnosis alone is unreliable, infection must be confirmed by laboratory investigation"
This is further supported in a 2006 paper about measles in the United Kingdom, where it is admitted that doctors do not look for or may not even recognize what to look for with a measles case. Clinical diagnosis is unreliable, and laboratory testing is required. Numerous other "causes" of the same fever and maculopapular rash are given such as rubella, parvovirus B19, enterovirus, scarlet fever, human herpesvirus 6, human herpesvirus 7, Kawasaki's disease, meningococcemia, toxic shock syndrome, dengue, HIV, secondary syphilis, and drug eruptions.
Measles in the United Kingdom: can we eradicate it by 2010?"As clinical experience of measles has declined, doctors in the United Kingdom may not consider the diagnosis nor recognise a case."
"Clinical diagnosis of measles has a low positive predictive value in settings such as the United Kingdom where the incidence is low.23 w15 Laboratory testing is required to confirm the diagnosis and to guide public health management (box 4).23 w15″
"Other causes of fever and maculopapular rash include rubella, parvovirus B19, enterovirus, scarlet fever, human herpesvirus 6, human herpesvirus 7, Kawasaki's disease, meningococcaemia, toxic shock syndrome, dengue, HIV, secondary syphilis, and drug eruptions."
"Every suspected case of measles should be notified. Clinical diagnosis is not reliable and it is therefore essential to return the oral fluid sample for laboratory confirmation."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1626346/

The reason why the CDC must alert healthcare workers when and how to look for measles cases is because healthcare workers do not actively look for measles cases nor would they know what one looks like if one walked into the office. Plus, just as the CDC assumes that those who are vaccinated are "protected" and can not possibly have measles, the physicians assume the same as well. This is called evidence of presumptive "immunity." All that one needs in order to be presumed "immune" to measles, according to the CDC, is one of the following: documentation of vaccination, laboratory evidence of "immunity," laboratory "confirmation" of measles, or being born before 1957:
Evidence of immunity"Acceptable presumptive evidence of immunity against measles includes at least one of the following:
- written documentation of adequate vaccination:
- one or more doses of a measles-containing vaccine administered on or after the first birthday for preschool-age children and adults not at high risk
- two doses of measles-containing vaccine for school-age children and adults at high risk, including college students, healthcare personnel, and international travelers
- laboratory evidence of immunity*
- laboratory confirmation of measles
- birth before 1957
https://www.cdc.gov/measles/hcp/index.html
We can see that this "presumptive immunity" trick pretty much negates anyone vaccinated as being a "true" measles case or of even being suspected of having the disease even if they match the clinical case definition. According to Chapter 7 of the CDC's Manual for the Surveillance of Vaccine-Preventable Diseases, the definition of a measles case that clinicians are supposed to follow is of an acute illness with a generalized maculopapular rash lasting greater than or equal to three days and a temperature of greater than or equal to 101°F along with cough, coryza, or conjunctivitis. However, in the fine print, the CDC states that the temperature does not need to reach 101°F and that the rash does not need to last equal to or greater than three days in order to "confirm" a measles case, thus making those clinical descriptors essentially meaningless. Also, in the case that someone tests positive for measles via "virus isolation," PCR, or serology tests, if they have been vaccinated with MMR within 6 to 45 days, they are not considered a measles case.
Case definition for case classification
Clinical description:
- An acute illness characterized by:
- generalized, maculopapular rash lasting ≥3 days; and
- temperature ≥101°F or 38.3°C; and
- cough, coryza, or conjunctivitis
Probable:
- In the absence of a more likely diagnosis, an illness that meets the clinical description with:
- no epidemiologic linkage to a laboratory-confirmed measles case; and
- noncontributory or no measles laboratory testing.
Confirmed:
- An acute febrile rash illness† with:
- isolation of measles virus‡ from a clinical specimen; or
- detection of measles virus-specific nucleic acid‡ from a clinical specimen using polymerase chain reaction; or
- IgG seroconversion‡ or a significant rise in measles immunoglobulin G antibody‡ using any evaluated and validated method; or
- a positive serologic test for measles immunoglobulin M antibody‡§; or
- direct epidemiologic linkage to a case confirmed by one of the methods above.
† Temperature does not need to reach ≥101°F/38.3°C and rash does not need to last ≥3 days.
‡ Not explained by MMR vaccination during the previous 6–45 days.
§ Not otherwise ruled out by other confirmatory testing or more specific measles testing in a public health laboratory.
As can be seen in the last highlight in the above fine print, a positive IgM serology test for measles must have not been ruled out by other confirmatory testing for different diseases first. This is due to the issue of a high rate of false positives as measles is not considered "endemic" in the US. Thus, as the risk of false positives are high, the laboratory testing for measles cases is supposed to be restricted to patients "most likely to have measles" which, according to the CDC, includes those who are unvaccinated, those who have a recent history of travel abroad, and those whose symptoms could not be determined with an alternate explanation. In other words, a measles diagnosis is seen as a last resort for a select few candidates, marking yet another trick utilized by the CDC to keep measles cases down and restricted primarily to the unvaccinated population. Interestingly, the CDC admits that many cases of febrile illness and rash may be reported as measles even when they are not "true" cases of measles. They even admit that some vaccinated individuals may be included in with the suspected cases. Thus, they state that laboratory testing must be done to confirm all suspected cases. However, the CDC then states that measles is difficult to "confirm" via laboratory testing in vaccinated individuals.
Because measles is a rare disease in the United States, even with the excellent laboratory tests available, false positive results for measles IgM will occur. To minimize the problem of false positive laboratory results, it is important to restrict case investigation and laboratory tests to patients most likely to have measles (i.e., those who meet the clinical case definition, especially if they have risk factors for measles, such as being unvaccinated, recent history of travel abroad, without an alternate explanation for symptoms, for example epi-linked to known parvovirus case) or those with fever and generalized maculopapular rash with strong suspicion of measles.
During a measles investigation when community awareness is increased, many cases of febrile rash illness may be reported as suspected measles, and the magnitude of the situation may be exaggerated if these cases are included in the absence of laboratory confirmation. This is particularly important as the investigation is ending; at that point, laboratory confirmation should be sought for all suspected cases. Occasionally, suspected cases may include vaccinated individuals. For these cases, laboratory confirmation may be challenging. An overview of diagnostic tools is described below."
The laboratory tests meant to "confirm" a measles diagnosis include "viral isolation," PCR, and IgM serology testing. However, negative results in both "viral isolation" and PCR are said not to rule out a measles case as the timing and collection of the specimen affect the results:
"Isolation of measles virus in cell culture or detection of measles RNA by RT-PCR in clinical specimens confirms the diagnosis of measles.
However, a negative virus isolation or negative RT-PCR results do not rule out measles because both methods are affected by the timing of specimen collection and the quality and handling of the clinical specimens."
While they admit to false negative results, the CDC fails to mention that the method used for "virus isolation" refuted itself with the measles "virus" in 1954 and it was shown to be an invalid pseudoscientific experiment. In fact, the results of any cell culture experiment are false results that do not equal "viral isolation." On top of that, PCR results are admittedly meaningless when a disease is not endemic as in the case of the measles due to the fact that, according to their own sources, a low disease prevalence rate generates high false positive results with PCR. This is a part of the prevalence problem for PCR that nullifies the results.
Regarding serology tests, the CDC states that no single serology test can confirm with 100% confidence every "true" measles case. False positive results are common in those with measles-like disease as well as false negative results in those previously vaccinated. Recently vaccinated individuals may come down with a measles-like disease, which means that an IgM serology test can not be relied upon for some strange reason in order to diagnose whether or not it is measles. The only way for a recently vaccinated person to become a "confirmed" measles case when they experience measles-like disease is to meet the clinical case definition and also be linked to someone else who was a laboratory "confirmed" measles case.
"There is no single serologic laboratory test capable of confirming with 100% confidence every true case of measles."
"Testing for measles-specific IgM from persons with rash and fever can produce false positive IgM results. As discussed above, false negative results can also occur in a previously vaccinated person."
"The occurrence of measles-like illness in recently vaccinated persons can pose particular difficulties. Fever and rash are known to occur 6–12 days post-vaccination in a small percent of vaccinated persons.[1] A positive measles IgM test cannot be used to confirm the diagnosis of measles in persons with measles-like illness who received measles vaccine 6–45 days before onset of rash due to the measles IgM antibody response to the vaccine. Specimens for viral isolation should be obtained in addition to serologic testing (see "Laboratory Testing" section above); isolation of wild type measles virus would allow confirmation of the case. In the absence of strain typing to confirm wild type infection, cases in persons with measles-like illness who received measles vaccine 6–45 days before onset of rash should be classified as confirmed cases only if a) they meet the clinical case definition and b) they are epidemiologically linked to a laboratory-confirmed case."

The CDC admits that it is difficult to diagnose any vaccinated person with measles due to the unreliability of the tests. Perhaps this is why most vaccinated individuals are presumed "immune" to measles and testing is saved for the unvaccinated? Regardless, the CDC acknowledges that even if a measles case is seen at a physician's office, it is most likely not a "true" measles case even if it meets the clinical definition. The only reason to suspect measles is if the person is unvaccinated and comes into contact with travelers from abroad. Granted, the CDC does say that cases of "high suspicion" should be investigated. However, this is only if other causes have been ruled out first, such as parvovirus, dengue, Kawasaki disease, scarlet fever, and rubella.
"In the measles post-elimination era, most cases of febrile rash illness seen in physician's offices that meet the clinical case definition will not be measles. However, health care providers should maintain a high index of suspicion for measles in clinically compatible cases especially among unvaccinated persons and among persons who recently traveled abroad or who have had contact with persons such as travelers or international visitors. In addition, not every sporadic measles case is linked to a known importation, so cases that raise high suspicion of measles, irrespective of associated risk factors, should be investigated for measles unless an alternative diagnosis is likely (e.g., known epidemiological link to a parvovirus case).
It is important to consider measles in the differential diagnoses of parvovirus, dengue, Kawasaki disease, and scarlet fever. In addition, when evaluating patients with suspected measles who have negative tests for acute measles infection, additional testing for rubella can be considered."
The list of potential diagnoses for the same symptoms of disease is much longer than what the CDC provided. Going back to the MN Department of Health, a more comprehensive list of diseases, both "infectious" and "non-infectious," presenting with measles-like symptoms is outlined. As these diseases all have similar features to measles, they all must be ruled out before a measles diagnosis can be made and "confirmed:"
"Providers should also consider other infectious and non-infectious etiologies that may cause fever and generalized rash, including:
- Rubella, Scarlet fever, Roseola infantum, Kawasaki disease, Erythema infectiosum (Fifth Disease), Coxsackievirus, Echovirus, Epstein-Barr virus, HIV, Pharyngoconjunctival fever, Influenza
- Dengue, Rocky Mountain spotted fever, Zika virus
- Dermatologic manifestations of Viral hemorrhagic fevers
- Toxic Shock Syndrome, cutaneous syphilis
- Drug reactions (e.g., antibiotics, contact dermatitis)

As can be seen from the above information, we are left with quite a few preconditions that must be satisfied in order for a new measles outbreak to be declared.
- The CDC must issue an alert for healthcare workers to start looking for measles cases.
- Testing should be limited to those who meet the case definition and are unvaccinated, have a recent history of travel abroad, and are without an alternate explanation for symptoms.
- Those with a history of previous measles "infection" or vaccination should be presumed to be "immune."
- Many clinicians do not know what a measles case looks like, so clinical diagnosis is unreliable, and it must be "confirmed" via unreliable tests.
- The long list of similar diseases presenting with the same symptoms must be ruled out via differential diagnosis first before "confirming" a measles case.
- A suspected measles case in someone vaccinated must meet the clinical case definition and be linked to a laboratory case in order to be a "confirmed" case.
With these preconditions firmly established, it is easy to see how the CDC can manufacture and steer a measles outbreak so that it appears as if it was instigated from outside of the US and spread through the unvaccinated. All they need is to alert clinicians in order to have them identify anyone unvaccinated who presents with nonspecific symptoms, such as a fever and a rash, that may have recently been a traveler or been in contact with one. They can then use unreliable laboratory tests to "confirm" that the case is measles rather than any of the other identical conditions it would have been pegged as prior to the alert. If someone who is vaccinated slips through as a suspected case, they make it difficult to confirm them as a measles case by blaming the unreliable tests and the vaccinated status and/or the presumed "immunity." Thus, a measles outbreak can be steered away from the vaccinated and pinned on any unvaccinated individual when they would have normally been diagnosed with any of the other conditions presenting with a fever, a maculopapular rash, and nonspecific symptoms of disease. Voila! The CDC gets to declare a measles "outbreak" in the unvaccinated instigated from contact coming outside from an "endemic" country. Now that the curtain has pulled back, and the trick has been exposed, it is time to cancel this magic show once and for all.
This article originally appeared on ViroLIEgy's Antiviral Substack.
11 Feb 2024 | 4:35 pm
Uncovering the Pseudoscience of ViroLIEgy with The Lawful Rebel
Recently, I was invited back onto the Living outside the Matrix podcast with Nigel Howitt. We had a very productive conversation covering many different aspects of the fraud of virology. It was a pleasure to be back on to speak with Nigel. I hope that you enjoy our latest conversation!
In this episode of "Living outside the Matrix" Nigel Howitt interviews Mike Stone, who uncovers the pseudoscience of virology. Mike is an inspirational example to every non-professionally-qualified thinker and seeker of truth, in that he demonstrates a rational approach to acquiring knowledge. His reasoning uses the method is logic, as he looks for evidence, and evaluates claims according to the soundness of their logical argument (if any). His website www.viroliegy.com is an outstanding resource and compendium of information that totally dismantles the illusion that virology is a credible science.
For the show notes and additional resources go to https://lawfulrebel.com/psuedoscience-of-virology
To find out more about how to discern truth and take control of your life visit https://lawfulrebel.com/
To sign up for the Lawful Rebel Newsletter go to https://lawfulrebel.com/
Follow Lawful Rebel on these platforms:
Bitchute – https://www.bitchute.com/channel/lawfulrebelcom/
Odysee – https://odysee.com/@LawfulRebel:0b
Youtube – https://www.youtube.com/c/LawfulRebelTV/featured
2 Feb 2024 | 3:38 pm
Virology Interview With Lies Are Unbekoming
I was recently asked to participate in a written interview about virology for the Substack "Lies are Unbekoming." It was presented to me as "a written Q&A format" that is "an old form 'analog' format whose time has returned as it gives the interviewed time to consider their responses in depth (and provide links to other work), and it gives the readers time to ponder and reflect on the answers." I couldn't have agreed more, as I regularly give my best responses when having the time to think, reflect, and gather my thoughts and evidence. I was very intrigued as I have always wanted to do a written interview. I was not disappointed as the questions were thought-provoking and hit on the major points underlying the fraud of virology. I hope you all enjoy!  – Mike Stone
– Mike Stone
I published Virus last month and the comments section exploded.
I've had more comments on this article than any other of the 350+ posted so far.
https://unbekoming.substack.com/p/virus
I pinned my comment in that article saying this:
I think the best description of my current state on this question is:
Covid and its vaccine was brought to me by the same charlatans that created virology. On that basis, what are the chances that virology is wholly or substantially untrue and corrupt. I think pretty damn high. Bordering on a certainty.
On that basis I would like to try to figure out what and where the untruths are. Cowan makes some very specific points. If they can be refuted, then I welcome the refute.
This is important stuff. The whole globalist plan is built around the idea of public health. The primary threat to global public health is viruses, we are told. The primary solution to that threat are vaccines (a virology product).
So, said another way, the whole world is now being run on ideas birthed out of virology. If there is any subject at all, that merited rigorous interrogation, seeking its truth; this is it.
In my quest to understand more I came across Mike Stone and his Substack.
https://mikestone.substack.com/
I've spent quite a bit of time reading his articles and have decided that I found a subject matter expert. He thinks and writes with a great critical mind, is widely and deeply read, and supports all his points with references. And, just for good measure, he can explain this stuff to a layperson.
So, I approached him for a written interview and as you will see below, I think he has produced something that is frankly magnificent.
I think, like Cowan, in my Virus article, Stone lays out considerable evidence for his views and positions. To the extent that one wants to disagree or dispute these positions, I think the onus is on us to refute his evidence with better evidence.
I've always maintained that if the inputs cannot be refuted, then the output stands.
In the interview Stone quotes William Summers from a 2014 article Inventing Viruses:
"In a very real way, a virus is what virologists say it is."
This reminds me of a great documentary I watched many years ago:
https://www.imdb.com/title/tt0487092/
Where a couple buy a painting at a garage sale and then spend years trying to get it authenticated as a Pollock. At the end of the documentary, the pre-eminent expert on Pollock's paintings is interviewed, and he says, with an edge in his voice:
"It's a Pollock when I say it's a Pollock."
This issue, encompassing Virology, Immunology, and Vaccinology, is a matter of gatekeeping. The gatekeepers, both individuals and institutions, have proven themselves to be untrustworthy.
Born of this justified distrust, it is now only fair and reasonable to question Virology, for that is what they, the Gatekeepers, have deservedly brought onto themselves.
Without further ado, and with much gratitude and appreciation I give you Mike Stone.
[Note: Any errors in the footnotes are mine and are based on the Official Story.]
Tell us a bit about your background and journey to this point.Regarding my educational background, I earned my BA in Exercise Science in 2004 from the University of Northern Iowa. I was a personal trainer for a few years until a back injury in 2007 unfortunately left me unable to continue pursuing that career. I adjusted by becoming a Health Coach, which utilizes a conversational approach focused on reflective listening to help clients to discover the root issues affecting their health. We work to uncover and ignite the intrinsic motivation within to help clients achieve success in accomplishing their health-related goals.
Regarding my awakening, there are three major events that woke me up to the madness that is our "healthcare" industry as well as the fraud of germ "theory" and virology. The first was dealing with shady practices within the medical industry while trying to resolve issues with chronic pain stemming from my back injury. This over 10-year journey left me frustrated and disenfranchised with our "healthcare" system, and it nearly killed me with pain medications.
The second event was the birth of my son in 2013. Upon taking him for his childhood vaccinations, he experienced bad reactions on two separate occasions, and these reactions woke me up to the vaccination lie. We immediately stopped vaccinations after my son's first birthday, and this compelled me to start to really examine the approach that our system used to make us "healthy."
The most pivotal event that shook me awake was when my mother-in-law finally came to the US to live with us in 2017. Unfortunately, due to a perfect storm of circumstances, she fell ill within a few weeks of her arrival. My mother-in-law was then given multiple inaccurate diagnoses as to the cause of her illness, and she was subjected to toxic treatments that left her in a worse stare than before. I witnessed the system murder my mother-in-law over a three-year period, and my faith in it was utterly shattered.
However, during this time, I began to research how accurate disease diagnosis was due to a fraudulent HIV test result my mother-in-law had received. This led to my learning about the HIV/AIDS lie due to the work of Dr. Stefan Lanka, the Perth Group, David Crowe, Kary Mullis, Peter Duesberg, Jon Rappoport, and many others. I learned that HIV had never been purified and isolated nor ever demonstrated to be the cause of AIDS. Once the HIV/AIDS domino fell, I started to understand that the same issues with HIV were present in all "viruses." While I researched quietly in the background for my own knowledge, the "Covid-19 pandemic" created a sense of urgency within me to speak out. I started ViroLIEgy.com (and eventually the Antiviral Substack) in order to bypass censorship and reach a wider audience in order to spread awareness.
Why is the process of viral isolation critical in the study of viruses and their impact on human health?'The issue of isolation is of major importance in order to actually study a thing properly. If a researcher is going to examine and attempt to learn about the particles that they believe are a "virus," they would need to have only those particles that they believe to be the "virus" on hand. They would need to separate the assumed "virus" from everything else that is contained within the fluids of the host. This includes host materials and constituents, bacteria and fungi, cellular debris and extracellular vesicles, and any other microbes or organisms both known and unknown. Only then could they actually study the assumed "viral" particles effectively by determining which ones they believe are the assumed "virus" from a sea of similar and identical particles of the same size and density. Only then would the researchers have a proper independent variable (i.e. the cause – the assumed "viral" particles) to vary and manipulate during experimentation in order to determine what influence it has on the dependent variable (i.e. the effect – the specific symptoms of disease). Only then could they attempt to prove pathogenicity naturally by subjecting a healthy host to nothing but the isolated particles believed to be the "virus" without any other confounding variables present.
The problem for virology is that they have completely debased the meaning of the word "isolation." Instead of separating one thing from everything else, they add multiple things together into a petri dish and assume that a "virus," which they have never isolated or identified prior to any experiment taking place, exists within the fluids. In other words, rather than isolation via subtraction as it should be done logically, virologists do "isolation" via addition which is not logical in the slightest. This process consists of taking the unpurified fluids containing host materials and other contaminants and adding them to a solution called "viral" transport media. This solution itself is a mixture of nutrients, chemicals, and fetal bovine serum (the blood from the heart of a baby cow). This is then added to a cell culture which is also contained in its own media consisting of similar components. The cell utilized is usually taken from the kidneys of an African green monkey, but they also use cells from dog kidneys, cells from cancer patients, and cells from aborted fetuses. Antibiotics and antifungals known to be toxic to cells, especially kidney cells, are also added at various stages. The researchers will incubate this toxic unpurified mixture until they see signs of a cell dying, and then claim that the cell death, known as the cytopathogenic effect (CPE), was brought about by the "virus" that was assumed to exist, but never identified, from the start.
One major problem for virologists is that this cytopathogenic effect is known to occur due to various factors, including:
- Bacteria
- Amoeba
- Parasites
- Antibiotics
- Antifungals
- Chemical contaminants
- Age and cell deterioration
- Environmental stress
Thus, this effect that is used to claim that a "virus" is present within a cell culture is not specific to any "virus" and does not require any "virus" whatsoever as an explanation.
Regardless, here is how the cell culture process was described by Zhou et. al in one of the foundational papers for "SARS-COV-2:"
"Human samples, including oral swabs, anal swabs, blood and BALF samples were collected by Jinyintan hospital (Wuhan, China) with the consent of all patients and approved by the ethics committee of the designated hospital for emerging infectious diseases. Patients were sampled without gender or age preference unless indicated. For swabs, 1.5 ml DMEM containing 2% FBS was added to each tube. The supernatant was collected after centrifugation at 2,500 rpm, vortexing for 60 s and a standing period of 15–30 min. The supernatant from swabs or BALF (no pre-treatment) was added to either lysis buffer for RNA extraction or to viral transport medium for isolation of the virus. The viral transport medium was composed of Hank's balanced salt solution (pH 7.4) containing BSA (1%), amphotericin (15 μg ml−1), penicillin G (100 units ml−1) and streptomycin (50 μg ml−1). Serum was separated by centrifugation at 3,000g for 15 min within 24 h of collection, followed by inactivation at 56 °C for 1 h, and was then stored at 4 °C until use.
Virus isolation, cell infection, electron microscopy and neutralization assayThe following cell lines were used for virus isolation in this study: Vero E6 and Huh7 cells, which were cultured in DMEM containing 10% FBS. All cell lines were tested and free of mycoplasma contamination, submitted for species identification and authenticated by morphological evaluation by microscopy. None of the cell lines was on the list of commonly misidentified cell lines (by ICLAC).
Cultured cell monolayers were maintained in their respective medium. The PCR-positive BALF sample from ICU-06 patient was spun at 8,000g for 15 min, filtered and diluted 1:2 with DMEM supplemented with 16 μg ml−1 trypsin before it was added to the cells. After incubation at 37 °C for 1 h, the inoculum was removed and replaced with fresh culture medium containing antibiotics (see below) and 16 μg ml−1 trypsin. The cells were incubated at 37 °C and observed daily for cytopathogenic effects. The culture supernatant was examined for the presence of virus by qRT–PCR methods developed in this study, and cells were examined by immunofluorescence microscopy using the anti-SARSr-CoV Rp3 N antibody that was generated in-house (1:1,000). Penicillin (100 units ml−1) and streptomycin (15 μg ml−1) were included in all tissue culture media."
As can be seen, at no point is a "virus" ever isolated from the fluids of the sick host and identified, which should be the very first step in this entire process. The cell culture is an invalid pseudoscientific experiment where the IV (the assumed "virus) is not identified until after the experiment takes place, and where the effect (CPE in this case) is known to be caused by factors other than a "virus." For more on this fraudulent process, please see this article.
Given the complexities in isolating viruses directly from bodily fluids, how do you assess the reliability of current viral isolation methods in accurately identifying and understanding viruses?The isolation methods are admittedly unreliable. The purification methods that are used for "viruses" such as centrifugation, filtration, precipitation, chromatography, etc. are all unable to separate the particles of the same size and density, even when they are combined together. From a 2020 review, it was stated that the technology to separate extracellular vesicles from "viral" particles does not exist:
"Nowadays, it is an almost impossible mission to separate EVs and viruses by means of canonical vesicle isolation methods, such as differential ultracentrifugation, because they are frequently co-pelleted due to their similar dimension [56,57]. To overcome this problem, different studies have proposed the separation of EVs from virus particles by exploiting their different migration velocity in a density gradient or using the presence of specific markers that distinguish viruses from EVs [56,58,59]. However, to date, a reliable method that can actually guarantee a complete separation does not exist."
Click to access viruses-12-00571.pdf
As there are both "viral" and "non-viral" particles that share the same size and density, they sediment and are co-pelleted together. A 2016 article stated that these particles are either similar or indistinguishable from "defective viruses."
"Because EVs are produced by virtually all cells, probably every viral preparation is in fact a mixture of virions and EVs. To study their respective functions, it is necessary to separate EVs and virions. This is very difficult with some viruses, such as retroviruses, because both EVs and retroviruses are comparable in size (EVs ranging from 50 to 100 nm, virions being ∼100 nm) and buoyant density (EVs: 1.13–1.18 g/L; most retroviruses: 1.16–1.18 g/L). Other membrane-derived materials may also have similar characteristics. Therefore, density gradients, which are often used to separate EVs from contaminating protein aggregates on the basis of differences in buoyant densities (40), are not always reliable for separation of EVs from viral particles."
"A growing body of evidence indicates that cells infected with enveloped or nonenveloped viruses release EVs that contain viral components. Here, we aimed to create awareness that virus preparations may never be pure but rather are contaminated with diverse subpopulations of EVs, and some of these EVs may be either indistinguishable from or very similar to so-called defective viruses."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4995926/
Thus, the mixtures claimed to be "purified" and isolated "viruses" are neither as there are many similar and identical particles remaining within the sample even after purification procedures are performed. This means that it would be impossible to determine which particles are the assumed "virus" and which particles are not, especially when dealing with a "novel virus." For more on the purification procedures, please see these articles. For more on the inability to separate "viruses" from similar and identical particles such as "exosomes," please see these articles.
Given the historical debate a about whether filterable 'viruses' were microscopic entities or merely effects of toxins, what implications does this have for our current understanding of viral pathogenesis?The issue is that the debate over what a "virus" is centered on a concept that was not based on any observed natural phenomenon. According to Field's Virology textbook, the concept of the invisible "virus" was born once the researchers studying bacteria realized that they were unable to satisfy Koch's Postulates, the criteria considered absolutely necessary to fulfill in order to prove that microbes cause disease:
"These studies formalized some of Jacob Henle's original ideas in what are now termed Koch's postulates for defining whether an organism was indeed the causative agent of a disease. These postulates state that (a) the organism must be regularly found in the lesions of the disease, (b) the organism must be isolated in pure culture, (c) inoculation of such a pure culture of organisms into a host should initiate the disease, and (d) the organism must be recovered once again from the lesions of the host. By the end of the 19th century, these concepts became the dominant paradigm of medical microbiology. They outlined an experimental method to be used in all situations. It was only when these rules broke down and failed to yield a causative agent that the concept of a virus was born."
As they were unable to identify and blame bacteria, the researchers assumed that there must be something even smaller than bacteria that were the cause of disease. This idea of a filterable "virus" was born primarily from the work of three men: Dmitri Ivanovski, Martinus Beijerinck, and Friedrich Loeffler. Their work consisted of creating experimental disease using various unnatural methods that damaged the host. You can find out more detail on their studies in the article "The Virus Concept."
The concept of the "virus" existed only as an idea. The "virus" is a fictional entity used to explain disease. As there was no observation of any "virus" in nature as well as no verified independent variable in purified and isolated "viral" particles to study and experiment with, "viral" pathogenesis is a fraudulent model that was established based upon various forms (cell cultures, antibodies, electron microscopy, genomes) of indirect pseudoscientific evidence.
With the evolving definition of viruses throughout the 20th century, what were the key challenges and controversies that scientists faced in reaching consensus on what constitutes a virus?The "virus" concept evolved greatly throughout the first half of the 20th century as the researchers had no actual physical entity that they were working with as well as no standardized methods with which to perform their research. Thus, there were many conflicting and contradictory ideas and findings throughout this period. Some believed "viruses" to be either toxic proteins or enzymes. Others, as documented by biochemist and historian of science Ton van Helvoort's 1996 paper When Did Virology Start?, believed "viruses" to be simply smaller bacterial forms. As the "virus" concept lacked clarity and certainty over the first half of the 20th century, and the link between bacteriology and "viruses" was so strong at this time, these unseen entities were not considered conceptually distinct from bacteria:
"I have come to believe that, despite its widespread appearance in textbooks and journals of that era, the early concept of the "filterable virus" lacked clarity and certainty. More importantly, I also believe that during the 1930s and 194Os, the links between the study of filterable viruses and bacteriology were so strong that viruses were still considered merely another form of bacteria-not conceptually distinct, as they now are."
With a lack of standardized methods, the findings of effects associated with a specific "virus" from one group of researchers could not be reproduced nor replicated by other groups of researchers. In fact, results were often contradictory towards what was considered established evidence. As such, researchers could not agree on what exactly a "virus" was nor whether the experimental evidence offered was in fact valid or not. A great summary of this rift was presented in a 1999 essay On the history of early virus researchby Karlheinz Lüdtke:
"With the "filterable" virus, something had been discovered which, according to the traditional concepts, which after all had mostly proved their worth in research into infectious diseases, could not be described in a way that all researchers could have shared. Very different interpretations of the nature of this phenomenon arose, which were put forward against each other. No experimental evidence for this or that concept, which all researchers should have accepted, could be presented by any side. In other words, the decision as to whether this or that explanation most accurately expresses the "true" nature of the virus could not be "objectified" empirically. Every version of the interpretation of the phenomenon remained open to attack, facts presented to the expert public could often be reinterpreted into fictions by opponents, who brought into play the dependence of the findings on the conditions of observation, the local situation of the experiments, the research-related nature of the attributions of characteristics, etc. as sources of error. For example, findings often reported by certain virus researchers at the time were not confirmed by other researchers as a result of their own experiments, or the observations could not be reproduced by all scientists working with the virus. Often, findings to the contrary were reported, or the findings that had been examined were considered artefacts. As with justification, reasons of various kinds could be invoked to reject the positions debated. Findings that were used to empirically confirm a suspected connection were often soon joined by negative findings reported by other researchers. However carefully and deliberately the techniques used in the experiments were employed, and despite the fact that each party could offer credible reasons for defending their respective positions and provide empirical evidence – which explains why "the various opponents 'constructed' widely diverging research objects which they identified as the 'virus'" (van Helvoort 1994a: 202) – at no time did they offer compelling reasons that would have led the other party to finally abandon artifact accusations."
In a 2014 article Inventing Virusesby William Summers, a retired Professor of Therapeutic Radiology, Molecular Biophysics & Biochemistry, and History of Medicine, he stated that "viruses" are whatever a virologist says that they are, and that the concept is continually reinvented.
"In a very real way, a virus is what virologists say it is. It is a product of the way virologists talk about viruses—that is, the way facts about viruses are organized in their discourse. It can be said that virologists invent (and continually reinvent) the concept of a virus as part of the normal progress of their science."
Sharing similar sentiments as van Helvoort, Summers stated that the "virus" concept is an unstable one that "evolved," not due to an accumulation of facts, but rather due to an ongoing reformulation of the "virus" concept on the basis of "scientific" focus at a given time. This reinvention was determined by technological advances rather than scientific understanding. Thus, the answer as to what a "virus" is will depend upon the discourse at the time more so than the "known" characteristics of "viruses:"
While there was plenty of data about "viruses" accumulated in the early 1900s, even virologist Thomas Rivers acknowledged that the accumulated data was "distinctly lacking in quality," and that "enough reliable data have not been acquired to establish the nature of the viruses." It wasn't until 1957 when French microbiologist Andre Lwoff smashed together highly debated competing concepts regarding the nature of bacteriophages, claiming that phages were "viruses" of bacteria, that a manufactured "consensus" opinion was formed. Animal and human "viruses" were then modeled after bacteriophages.
How does Karl Popper's principle of falsifiability apply to the field of virology, and what are its implications for distinguishing between scientific hypotheses and pseudoscientific theories?The concept of falsifiability was introduced by scientific philosopher Karl Popper in 1935 in his book The Logic of Scientific Discovery. Essentially, what falsifiability means is that, in order for a hypothesis or theory to be scientific, it must have the ability to be disproven. Someone should be able to conceivably design an experiment that could prove the hypothesis or theory wrong. If a hypothesis or theory is capable of being proven wrong and yet it is supported by experimental evidence of its truth, then it can be considered as a scientific hypothesis or theory. As explained by Popper in his 1963 book Conjectures and Refutations, falsification was an attempt to draw a line between science and pseudoscience.
For virology to be considered a scientific field, the underlying hypotheses must be falsifiable. For example:
Hypothesis: If a "coronavirus" is the cause of atypical pneumonia, then it will cause the same symptoms of disease when healthy hosts are exposed via aerosol.
This is a falsifiable hypothesis, as long as purified and isolated "viral" particles are obtained and identified prior to experimentation, as it can be tested experimentally and falsified when healthy hosts do not come down with atypical pneumonia. However, it becomes an unfalsifiable hypothesis if the "coronavirus" is allowed to be the cause of atypical pneumonia even though it is shown experimentally not to produce the same disease in animals and humans.
Virology is full of unfalsifiable concepts that allow for falsified hypotheses to remain as supporting evidence for the unproven "theory:"
- The concept of the asymptomatic carrier is an unfalsifiable concept as it allows for supposed disease-causing agents to be considered as such even when they are "found" not causing disease.
- Relying on "antibodies" and the "immune" system to explain away why people are not getting sick through experimentation creates an unfalsifiable scenario to explain away contradictory results, as many have tried to do when brushing off the findings of Milton Rosenau's Spanish flu experiments.
- Allowing for the presence of a "virus" in a cell culture even though no cytopathogenic effect is observed is another unfalsifiable concept, as this effect is supposed to signal the presence of a "virus" in a culture.
- The existence of "virus-like" particles such as multivesicular bodies, clathrin-coated vesicles, the rough endoplasmic reticulum, and/or other extracellular vesiclesfound in those without disease, even though these same particles are identified as "pathogenic viruses" when seen in those with disease.
By looking at the examples of unfalsifiable concepts present in virology, it should be clear to see how variable and vague the concepts of virology truly are. As stated by Oxford Reference, pseudoscience "provides no room for challenge and tends to dismiss contradictory evidence or to selectively decide what evidence to accept." They conclude that pseudoscience is "nothing more than a claim, belief, or opinion that is falsely presented as a valid scientific theory or fact." There is an inability to challenge virology experimentally as there are numerous unfalsifiable concepts available as escape hatches that can be used by virologists in order to dismiss contradictory findings that should falsify the hypothesis. Thus, virology is a pseudoscience.
Considering the variability and non-specific nature of antibody responses, how reliable are antibody tests in confirming or refuting the presence of viral infections?Antibody tests are unreliable and the results are uninterpretable. For example, early during the "Covid pandemic," the CDC stated that antibody tests could be wrong over 50% of the time, and that the results from these tests should not be used for policy decisions as they are not accurate enough.
"The CDC explains why testing can be wrong so often. A lot has to do with how common the virus is in the population being tested. "For example, in a population where the prevalence is 5%, a test with 90% sensitivity and 95% specificity will yield a positive predictive value of 49%. In other words, less than half of those testing positive will truly have antibodies," the CDC said."
Another article from CNN from May 2020 stated that antibody results cannot be trusted as the tests are unreliable due to a high number of false positives.
The tests can't be trusted: Then there's the fact that while antibody tests are crucial in determining past exposure to coronavirus, not all available antibody tests are reliable. Some antibody tests had high rates of false positives in screenings performed by a consortium of California laboratories. A false positive means someone would be told they'd been previously exposed to coronavirus when they had not.
https://www.cnn.com/2020/05/22/health/immunity-passport-coronavirus/index.html
The reason that the tests are not accurate, as well as non-specific as stated in your question, is due to the fact that, like "viruses," antibodies have never been purified and isolated directly from the fluids of a host and had the functioning determined via the scientific method. The tests are not calibrated and validated to something that exists and has any real scientific meaning. Thus, the results vary and are essentially meaningless. For more on antibodies, please see these articles.
How does the existence of non-cytopathogenic viruses, which do not produce a cytopathic effect in cell cultures, complicate the process of virus detection and identification?The existence of non-cytopathogenic "viruses" is one of the many unfalsifiable concepts related to virology. The cytopathogenic effect is supposed to be the sign that a "virus" is present within a culture. According to Axion Biosystems, looking at the damage a "virus" causes to a cell is a practical way of "seeing" and indirectly measuring a "viral infection." John Franklin Enders, who coined the term cytopathogenic effects while working on polio tissue cultures in 1949, described it as such in his 1954 paper Cytopathology of Virus Infections:
By "viral cytopathogenicity" is understood the capacity to induce any demonstrable departure from the normal either in the morphological or functional properties of cells. Cellular changes are referred to as "cytopathogenic effects" of the virus or "cytopathic" changes.
These effects are attributed to the presence of a "virus." Enders further discussed this process in his 1957 paper Comments on Viral Cytopathogenicity:
"The multiplication of viruses, so far as is known, is dependent upon an extremely intimate association with living cells of higher forms. During the course of viral multiplication, which takes place within the cell, the cell is frequently, although not invariably, injured or destroyed. This capacity of viruses to injure and destroy cells, i.e., to cause cellular disease, is now often referred to as "viral cytopathogenicity," and the resultant changes are designated as "cytopathogenic effects."
The CPE is supposed to be a sign of "viral" multiplication and the ability to cause cellular disease. The culture is observed under a microscope in order to see if CPE is present or absent. If a cell culture does not produce this effect, it is supposed to be negative for the presence of a "virus." This is how the cell culture, if it was a valid scientific experiment based upon a valid hypothesis, should be falsified. However, virology has allowed for the lack of any observable CPE to still signify a "viral" presence if other indirect methods (antibody results, hemadsorption tests, PCR) "show" the "virus" is in there. Thus, we have an unfalsifiable concept for a pseudoscientific experiment bolstered by the usual escape hatches.
What would you like to tell people about exosomes, particularly in the context of virology and disease transmission?The entities referred to as exosomes are just another name that has been given to the same random particles of cellular debris claimed to be "viruses." The particles were actually considered to be nothing but cellular debris when they were originally discovered. However, it was eventually decided to give these particles, which are identical to "viruses" in nearly every way, the job of transporting proteins and mRNA throughout the body. Thus, instead of being cellular garbage bags, these random particles created from cell cultures without "viral" material present, were given an unobservable, hypothetical job. In other words, exosomes are just another fictional concept explaining the same exact particles observed after culturing.
Is the science around exosomes solid and reliable, or do you see elements of pseudoscience influencing the research and understanding in this area?The same problems that occur in virology also occur in exosome research. The researchers are unable to purify and isolate the particles of the same size and density from each other. Thus, there is no valid independent variable to use for any experimentation. This excerpt from the article Extracellular Vesicles and Viruses – Two Sides of the Same Coin? details the problem brilliantly (the article link is sadly broken):
"How can we be sure that we are isolating and quantifying extracellular vesicles rather than enveloped viruses present in the sample? Equally, how can viral researchers know that they are not detecting similarly sized non-viral vesicles or empty vectors during vaccine production?"
As exosomes and "viruses" are unable to be separated from each other (as they are the same particles), there is no way to be able to study either independently, distinguish them from any of the other particles, or to characterize the particles properly. A 2019 study highlighted the issues of the similarity of composition and function between exosomes and "viruses" while stating that there are particles that blur the line even further by containing both host and "viral" components, making it impossible to classify them as either one or the other.
"The generic characterization of extracellular vesicles could also be used as a descriptor of enveloped viruses, highlighting the fact that extracellular vesicles and enveloped viruses are similar in both composition and function. Their high degree of similarity makes differentiating between vesicles and enveloped viruses in biological specimens particularly difficult."
"However, as previously reviewed, exosomes and viruses do not conform to strict definitions [22]. Intermediate particles exist on the spectrum between virus and exosome that contain both host and viral components, making it nearly impossible to classify these vesicles as either defective viruses or exosomes that contain viral components [22]. Intermediate particles are often classified as a virus or exosome derivative, depending on the preference of the investigator, but once these vesicles deviate from strict definitions they may be more accurately defined as an assortment of lipid-encased particles that cannot be easily differentiated [22]."
When one investigates the origins of the exosome concept, it is clear that researchers found the exact same "viral" particles in their cultures that contained no "viral" materials. Rather than allow these findings to tear down the "virus" lie, a new fictional entity was created in order to explain away the contradictory findings. For more on the exosome fraud, please see these articles.
Based on your critique of conventional methods used in studying viral transmission, could you elaborate on what you see as the major flaws in the current understanding of how viruses are transmitted between individuals?"I would say that the major flaws begin with the assumption that one human can transmit disease to another human (or animal to human), and that this occurs due to invisible floating lifeless boogeymen that somehow enter a body, bypass any defenses, and highjack the cells in order to replicate and cause disease. This is not a naturally observed phenomenon. No one has ever witnessed one human passing a "virus" on to another human in order to cause disease. As will be addressed in the next question, there is no scientific evidence demonstrating that any such transmission ever occurs.
Can you comment on the history of experiments that failed to demonstrate virus transmission. Could you elaborate on why you believe these experiments are critical to understanding the current state of virology?There have been numerous attempts to take the fluids of a sick person, as well as pure cultures of bacteria, in order to try and make healthy hosts sick with the expected disease. These attempts regularly failed to produce disease in healthy hosts, especially when exposing them via natural routes of "infection" such as by breathing in aerosols, ingesting the pure cultures, or simply being around and interacting with those who are sick.
The most famous example is the Milton Rosenau Spanish flu experiments that took place on opposite coasts at different times. Keep in mind that the Spanish flu is considered the deadliest "virus" of all time. Volunteers at Gallops Island in Boston were subjected to one strain and then several strains of Pfeiffer's bacillus cultured from Spanish flu patients by spray and swab into their noses, throats and eyes. When these attempts failed to produce disease, new volunteers were inoculated with mixtures of other organisms isolated from the throats and noses of influenza patients. These attempts also failed, so the researchers used the blood from influenza patients and injected this into volunteers. When that failed to produce disease as well, thirteen volunteers were taken into an influenza ward and exposed to ten influenza patients each. True to form, this final attempt also failed to produce disease. These same experiments were repeated at Angel Island in San Francisco, and they, too, were entirely unsuccessful in transmitting the "virus" in every single case.
There are many other examples of the failed "infection" and "contagion" studies that I have collected in the Infectious Myth Busted series that include influenza, HIV, measles, polio, smallpox, and various bacterial diseases such as cholera, diphtheria, tuberculosis, glanders, and typhoid. Today, it is considered unethical to expose human volunteers to "infected" individuals via natural exposure routes. This is obviously because these experiments regularly failed to produce the desired results in the past. If they do attempt human challenge trials today, researchers use engineered cell cultured soups containing various additives and expose volunteers in unnatural ways, such as inoculating in the nose and holding this in place with a clothespin while lying down). However, even with these unnatural methods, they still fail to demonstrate human-to-human transmission of disease.
A 2003 review of the published experimental literature stated:
"Our review found no human experimental studies published in the English-language literature delineating person-to-person transmission of influenza."
This is true not just for influenza, but for all "infectious" diseases. Without the ability to demonstrate that one human can be "infected" and transmit disease naturally to another human, the germ hypothesis fails. In fact, based upon the available experimental evidence, the germ hypothesis has been repeatedly falsified.
In your writings, you challenge the established views on contagion and viral transmission. Could you propose an alternative model or method that, in your opinion, would more accurately explain and demonstrate the process of disease transmission?'I don't believe that disease can be transmitted from one human to another human. Beyond anecdotal stories of chicken pox and measles parties that have no scientific backing, the concept of disease transmission has been repeatedly demonstrated to be false. From my research, disease is multifactorial and develops by the actions of the individual. Thus, I lean heavily towards the terrain theory of disease. This theory, developed by Claude Bernard and Antoine Bechamp in the mid-1800s, states that dis-ease is not caused by invading pathogens from outside of the body. Instead, the dis-ease process begins from within due to the status of the internal environment of the body. If there occurs an imbalance within the internal environment and the body becomes too toxic, which could be brought about by a combination of many factors such as what we eat, drink, think, feel, etc., this would materialize in symptoms of dis-ease as the body intitiates a detoxification process in an attempt to restore balance.
There are many factors that can lead to dis-ease, such as:
- Increased exposure to air pollution
- Consuming non-organic, genetically modified, pesticide-laden foods
- Drinking unclean, fluoridated, and chlorinated water
- Living a sedentary lifestyle without regular exercise
- Consuming alcohol and recreational drugs
- Taking prescription medications and toxic vaccines
- Interrupted or inconsistent sleep cycle
- Lack of direct sunlight
- Long-term exposure to EMF's and other radiation
- Overabundance of stress
- Regular use of cleaning supplies and other chemicals
- Overaccumulation of heavy metals, plastics, or poisons
While it could be just one of these factors that initiates a detox, it is usually a combination of many of them acting together, along with the mistaken belief that the detoxification process, itself a healing phase, needs to be suppressed and stopped, that leads to worsening states of dis-ease. Unlike the germ "theory" which takes power away from the individual and chalks illness up to bad luck brought about by defective genes or outside invisible invaders, the terrain theory puts the power back onto the individual to take care of himself or herself in order to clean up the factors that are damaging the terrain. It is not on the doctor and the toxic pharmaceuticals to heal us (as if they truly could), it is within our own power to restore and create health. You can read more about the terrain theory here.
What are your thoughts on electromagnetic transmission of disease patterns. Can you explain how this challenges the conventional understanding of disease transmission?While I do believe that electromagnetic radiation in the form of EMF's and different frequencies such as 5G can impact our health, I have not done enough research into the topic in order to speak on it in-depth. However, I have heard very good reviews on the book The Invisible Rainbow by Arthur Fristenberg, so I would recommend anyone interested in exploring the connection between disease outbreaks and the introduction of electromagnetic radiation to begin by reading that book.
What are your thoughts on informational transmission from person to person? If viruses do not exist and as such are not a means of information transfer, do you think there is evidence for other forms of information transfer?I think that it is a vastly understudied and unexplored area. While I do not believe that disease can be transmitted from one person to another, there may be some form of communication that initiates a detox in the same way that women can sync up menstrual cycles. It could be brought on by a visual and/or auditory cue in the same way that one yawns after witnessing another person yawn. While yawning appears contagious, no one is claiming that a "virus" is being transferred from the first person to the second. There are visual and auditory cues that are picked up on, and if one needs to yawn, the body will initiate the process. This could be the same for someone whose body is in a toxic state and witnesses another person going through a detox. The visual and auditory cues could potentially initiate the individuals own cleansing response if the necessary internal conditions are present. It is definitely something that needs to be explored further over invisible boogeymen.
How can we understand childhood illnesses such as measles and chickenpox without attributing them to viruses? What alternative explanations might exist?I tend to view chickenpox and measles similarly to how Rudolf Steiner viewed childhood diseases. Steiner seemed very much inclined to believe that disease occurred from spiritual conflict from within and that childhood diseases were caused by the child adapting to the physical world. He believed that the mind played a significant role in "catching" and preventing disease. He felt that the symptoms of disease experienced by children were a natural part of childhood development as the child ages.
"Rudolf Steiner generally portrayed the traditional childhood diseases as signs, aids, trials, and accompaniments of the natural process of child development and maturing immune systems."
Here is a direct quote from Steiner from the same source.
"The risk of infection is actually great in diphtheria-related disorders, but why? It is because they develop in direct connection with learning to speak, and occur therefore most widely in children aged between two and four. After this age children are less susceptible. But every process in the human organism that arises in the normal course of things at any particular period can also arise abnormally. This process, therefore, that is really simply a natural process of childhood development can also occur at a later age, albeit in a somewhat modified form, a metamorphosis. When diphtheria occurs at a later age this is in a sense an infantile condition that works on in a person."
These dis-eases very well could be a part of a normal developmental process that children go through, just as acne tends to be a normal condition when kids start going through puberty.
Regarding historical practices like measles parties for local children to 'catch' measles and recover simultaneously, what is a better explanation of the 'catching' process in your view, especially without the virus concept?The issues with chickenpox and measles parties is that they are anecdotal. There is no scientific evidence experimentally demonstrating that one child can pass on either condition to another child. Just because kids go through the same detoxification process via skin eruptions does not mean that this was the result of an "infectious virus" transmitted between them. We wouldn't claim that because some kids at a party started breaking out in pimples after attending, that this was caused by other pimply-covered kids who were at the same party. We understand that kids at a certain age start to experience acne breakouts, whether due to hormones, stress, the foods that they eat, etc. There is no need for a pimple vaccine to stop the pimple "virus." Eventually, the skin will clear up, especially if the underlying issues are addressed.
The causes for these detoxification symptoms in children is most likely multifactorial. It likely involves the environment that the children are in, the age and development of the child, the foods/drinks they consume, the mental and physical stressors that they experience, etc. As stated earlier, there could be some sort of visual and/or auditory cues that may help initiate this process in some children if the body requires it. However, it could just be that they are all at the same age and at similar developmental cycles, thus they experience the same detoxification protocol around the same time. One thing that is for certain is that there is no scientific evidence that either chickenpox or the measles are caused by a "virus" and that these symptoms can be transmitted from one child to another. Please click on the links for more on chickenpox and measles.
How can interested individuals stay updated with your latest work and research in the field of virology?For those who are interested and want to follow my work, they can do so via my two sites.
Thank you for your interest and support.
Absolutely! The key authors I would recommend include:
- Dawn Lester and David Parker's What Really Makes You Ill?
- Dr. Mark Bailey's A Farewell to Virology
- Dr. Tom Cowan's The Truth About Contagion
- Virus Mania by Torsten Engelbrecht and Dr. Sam Bailey
- The Perth Group
- Ex-virologist Dr. Stefan Lanka
You can find plenty of other great authors and resources here.
Are there any documentaries or lectures you would suggest for a deeper insight into the problems and debates surrounding modern virology?Yes, I have plenty of documentaries as well as presentations and interviews.
I will highlight a few great presentations and documentaries for beginners.
- Dr. Jordan Grant's Science, Pseudoscience, and the Germ Theory of Disease
- Debunking the Nonsense
- The End of Germ Theory
- The End of Covid
- The Viral Delusion
- Virology's Unproven Assumptions
Additional information on the researchers that I mentioned within the interview was added by Lies are Unbekoming.
1. Dmitri Ivanovski (1864-1920) was a Russian botanist and microbiologist who is credited with contributing significantly to the foundations of virology. In 1892, he conducted pioneering research on the Tobacco Mosaic Disease. His most notable work involved experiments in which he demonstrated that a disease in tobacco plants could be caused by an agent smaller than bacteria, which could pass through a fine porcelain filter that was known to retain bacterial cells.
Ivanovski's discovery was instrumental in the later identification of viruses as a new class of infectious agents, fundamentally different from bacteria. His work laid the groundwork for further research by other scientists such as Martinus Beijerinck, who later coined the term "virus" to describe the infectious agent. Ivanovski's findings were critical in establishing the concept of non-cellular infectious agents, which challenged the prevailing scientific understanding of the time and opened up a new field of study in microbiology and infectious diseases.
2. Martinus Beijerinck (1851-1931) was a Dutch microbiologist and botanist who played a crucial role in the early development of virology and microbiology. He is best known for his work in identifying and understanding viruses as distinct entities separate from bacteria.
Beijerinck's most significant contribution came in 1898 when he studied the Tobacco Mosaic Virus, the same agent earlier researched by Dmitri Ivanovski. Beijerinck conducted experiments that confirmed Ivanovski's findings about the infectious agent's ability to pass through filters that would trap bacteria. However, Beijerinck went a step further in his interpretation. He concluded that the agent was not a bacterium, but something entirely different, which he called a "virus," a term derived from the Latin word for "poison."
Beijerinck's work established the concept of viruses as a new type of infectious agent, laying the foundation for the field of virology. He also made significant contributions in other areas of microbiology, including his work on nitrogen fixation by bacteria in soil, which had a profound impact on agriculture and our understanding of the nitrogen cycle.
Martinus Beijerinck is often considered one of the founders of virology and environmental microbiology due to his pioneering research and innovative approach to studying microscopic life.
3. Friedrich Loeffler (1852-1915) was a German bacteriologist and a pioneering figure in the field of microbiology, particularly known for his contributions to the study of infectious diseases. He is best recognized for his work in the discovery of the diphtheria bacillus (Corynebacterium diphtheriae) in 1884, alongside Edwin Klebs.
Loeffler's most significant contribution to virology came in 1898 when, together with Paul Frosch, he discovered the first animal virus, the agent causing foot-and-mouth disease in cattle. This was a landmark discovery because it was the first time a disease in animals was attributed to a viral pathogen. Their work involved demonstrating that the causative agent of foot-and-mouth disease could pass through filters that were known to retain bacteria, similar to the earlier discoveries in plant viruses by Dmitri Ivanovski and Martinus Beijerinck.
This discovery by Loeffler and Frosch not only had a major impact on veterinary medicine but also played a crucial role in the development of virology as a scientific discipline. It helped in establishing the understanding that viruses could infect animals as well as plants, thereby broadening the scope of virology significantly. Loeffler's work laid important foundations for the field and opened up new avenues for research into viral diseases.
4. Ton van Helvoort is a historian of science, particularly known for his contributions to the history of virology and microbiology. Unlike Dmitri Ivanovski, Martinus Beijerinck, and Friedrich Loeffler, who were scientists directly involved in the discovery and study of viruses, van Helvoort focused on the historical and philosophical aspects of these fields.
His work often involves analyzing the development of scientific concepts and the evolution of scientific understanding over time. One of his notable contributions is his research on the history of early virology, where he examines how the concept of viruses evolved from the late 19th century onwards. This includes exploring the debates and discussions among scientists about the nature of viruses and their role in diseases.
Van Helvoort's work is important for understanding the context in which scientific ideas develop and change. By examining the history of virology, he provides insights into how scientific communities negotiate and construct knowledge in fields that are new and evolving. His research contributes to a deeper understanding of the processes and dynamics that shape scientific disciplines.
5. Karlheinz Lüdtke is a historian of science, recognized for his contributions to the study of the history of virology and other scientific fields. His work, like that of Ton van Helvoort, focuses on the historical development of scientific concepts and the evolution of scientific understanding, rather than direct scientific discovery or experimentation.
Lüdtke's research often delves into how scientific ideas and theories have developed over time, examining the changes in scientific thought and the factors that influence these changes. He has contributed to the understanding of how scientific consensus is formed, how scientific theories evolve, and how various scientific, cultural, and social factors impact the development of scientific fields.
While not as widely known as some of the pioneering virologists like Dmitri Ivanovski or Martinus Beijerinck, historians of science like Lüdtke play a crucial role in contextualizing scientific advancements. They help us understand not just the scientific discoveries themselves, but also the broader context in which these discoveries were made, including the social, economic, and philosophical environments that shaped scientific research.
6. William Summers is a historian and professor emeritus known for his work in the history of science and medicine. He has a particular focus on the history of virology and microbiology, and his research has contributed to understanding the development and evolution of these scientific fields.
Summers' work often involves analyzing the historical context of scientific discoveries, exploring how scientific ideas are formulated, evolve, and are accepted or challenged within the scientific community. His research delves into the historical development of concepts in virology and microbiology, examining the changes in scientific thought and the influences that have shaped these disciplines over time.
His contributions are valuable for providing insights into the complex processes of scientific discovery and the evolution of scientific knowledge. By exploring the history of these fields, Summers helps to illuminate the paths that have led to our current understanding of viruses and microorganisms, as well as the societal and cultural impacts of these discoveries. His work underscores the importance of viewing scientific advancements not just as isolated events, but as part of a broader historical and cultural narrative.
7. Thomas Milton Rivers (1888-1962) was an eminent American virologist and bacteriologist, often referred to as the "father of modern virology." He made significant contributions to the field, particularly in the early to mid-20th century.
Rivers' impact on virology is notable for several reasons:
- Standardization of Virus Study: Rivers played a key role in standardizing the methods used to study viruses. He was influential in establishing virology as a distinct scientific discipline, emphasizing the need for specific techniques and approaches to study viral pathogens.
- Poliovirus Research: He made significant contributions to the understanding of poliovirus and was involved in early efforts to develop a vaccine against polio.
- Influenza Research: Rivers also conducted extensive research on influenza, contributing to the understanding of its causative agent and how it spreads.
- Laboratory Techniques: He developed and refined many of the laboratory techniques that are foundational to virological research, including methods of growing viruses in laboratory cultures.
- Leadership in Science: Rivers held prominent positions in scientific societies and institutions. For instance, he was the director of the Rockefeller Institute Hospital and served as president of the American Society for Clinical Investigation and the Society of American Bacteriologists.
- Education and Training: He was also known for his role in educating and training a generation of virologists, many of whom went on to make their own significant contributions to the field.
Rivers' work in virology helped lay the groundwork for many of the advancements in the study and treatment of viral diseases that followed in the latter half of the 20th century.
8. André Lwoff (1902-1994) was a prominent French microbiologist who made significant contributions to the field of virology and microbiology. He was awarded the Nobel Prize in Physiology or Medicine in 1965, shared with François Jacob and Jacques Monod, for their discoveries concerning genetic control of enzyme and virus synthesis.
Lwoff's major contributions include:
- Viral Lysogeny: Lwoff, along with his colleagues at the Pasteur Institute in Paris, extensively researched bacteriophages (viruses that infect bacteria). He was instrumental in elucidating the phenomenon of lysogeny, where a bacteriophage integrates into the bacterial genome and remains latent until it is later induced to enter a lytic cycle, where it replicates and causes cell lysis.
- Virus Classification and Biology: He made significant advances in our understanding of the nature and classification of viruses. Lwoff proposed criteria for defining viruses, which helped in distinguishing them from other biological entities.
- Research on Poliovirus: Lwoff's work on the poliovirus contributed to the understanding of viral replication and the development of polio vaccines.
- Influence on Molecular Biology: His work laid the foundations for many aspects of molecular biology, influencing the understanding of how genetic information is expressed and regulated in cells.
Lwoff's research was pivotal in demonstrating that viruses are genetic entities and can have complex interactions with their host cells. His work significantly advanced the understanding of viral life cycles and genetics, which has had lasting implications for virology, microbiology, and molecular biology.
9. Karl Popper (1902-1994) was an Austrian-British philosopher of science who is widely regarded as one of the most influential philosophers of the 20th century, particularly in the realm of scientific methodology and the philosophy of science. He is best known for his rejection of the classical inductivist views on scientific method in favor of empirical falsification.
Key Contributions and Concepts:
- Falsifiability: Popper's most significant contribution to the philosophy of science is the criterion of falsifiability. He argued that for a theory to be considered scientific, it must be able to be tested and potentially refuted by empirical evidence. In other words, a scientific theory should make predictions that could be shown to be false under certain conditions. If a theory is not falsifiable, then it falls into the realm of pseudoscience.
- Critique of Inductivism: Popper was critical of the traditional inductive reasoning approach in science, where generalizations are made based on a series of observations. He argued that no amount of empirical data could ever fully prove a theory, but a single counter-example is sufficient to falsify it.
- Problem of Demarcation: Popper's work on falsifiability stemmed from his attempt to solve the 'demarcation problem' – distinguishing between what is and isn't genuinely scientific. He used the criterion of falsifiability to demarcate scientific theories from non-scientific theories.
- Open Society: Apart from his contributions to the philosophy of science, Popper was also known for his political philosophy. In his book "The Open Society and Its Enemies," he critiqued the totalitarianism of his times and advocated for liberal democracy and the importance of critical discussion and debate in society.
- Philosophical Pessimism: Popper emphasized the 'fallibilism' of human knowledge – the idea that any of our beliefs could, in principle, be wrong. Thus, scientific theories should always be subjected to rigorous testing and should never be accepted as absolutely certain.
Karl Popper's ideas have had a profound impact on scientific thought, emphasizing the importance of critical testing and the tentative nature of scientific knowledge. His work continues to influence various fields, including philosophy, science, sociology, and political theory.
10. Milton Joseph Rosenau (1869-1946) was an American public health official, physician, and pioneering epidemiologist. He made significant contributions to public health, particularly in the areas of infectious disease control and preventive medicine.
Key Contributions and Aspects of Rosenau's Career:
- Public Health Work: Rosenau served as a director at the United States Hygienic Laboratory, the precursor to the National Institutes of Health (NIH). He played a crucial role in the development of public health services in the United States.
- Research on Infectious Diseases: Rosenau conducted important research on various infectious diseases, including tuberculosis, typhoid fever, and diphtheria. He was involved in the development of strategies for controlling these diseases, which had a significant impact on public health policies.
- Role in Epidemiology: He is noted for his contributions to the field of epidemiology, particularly in understanding the transmission and control of infectious diseases.
- The Spanish Flu Experiments: Rosenau is particularly remembered for his experiments during the Spanish Flu pandemic of 1918-1919. He conducted studies to understand the transmission of the influenza virus. In a series of experiments, healthy individuals were exposed to secretions from patients with influenza to see if the disease could be transmitted to them. These experiments, which failed to transmit the disease, were critical in shaping understanding of influenza transmission.
- Educational Contributions: Rosenau was also a professor and later the director of the Harvard School of Public Health. He was instrumental in training a generation of public health professionals.
- Publications: He authored several influential books and papers on public health and preventive medicine, which were widely used as textbooks and references in the field.
Rosenau's work in public health and epidemiology was pivotal in the early 20th century, contributing to the development of public health as a scientific discipline.
11. John Franklin Enders (1897-1985) was a prominent American biomedical scientist, often referred to as the "Father of Modern Vaccines." His work in virology and immunology led to significant breakthroughs in vaccine development and the study of infectious diseases.
Key Contributions:
- Cultivation of Poliovirus: One of Enders' most notable achievements was the successful cultivation of the poliovirus in non-neural tissue cultures. This breakthrough, achieved with colleagues Thomas Weller and Frederick Robbins in 1949, was a pivotal moment in virology. It enabled the large-scale production of the poliovirus and laid the groundwork for the development of the polio vaccine.
- Nobel Prize in Physiology or Medicine: Enders, along with Weller and Robbins, was awarded the Nobel Prize in Physiology or Medicine in 1954 for their work on culturing the poliovirus. This work was crucial in advancing the field of virology and vaccine development.
- Measles Vaccine: Enders and his team also played a key role in the development of the measles vaccine in the early 1960s. They were able to isolate and grow the measles virus, leading to the creation of an effective vaccine that has significantly reduced the incidence of measles worldwide.
- Research in Infectious Diseases: Apart from polio and measles, Enders conducted extensive research on other infectious diseases, including mumps and chickenpox. His techniques for growing viruses in tissue cultures revolutionized the study of infectious diseases.
- Impact on Public Health: The work of Enders and his team had a profound impact on public health, leading to the near-eradication of polio in many parts of the world and greatly reducing the prevalence of other infectious diseases.
Enders' contributions to virology and immunology, particularly his methods for culturing viruses, have had a lasting impact on medicine and public health, making him a key figure in the history of medical science.
12. Claude Bernard (1813-1878) was a renowned French physiologist and a pivotal figure in the history of medicine and biology. He is best known for his work in the field of physiology and for introducing the concept of homeostasis, as well as his methodological approach to scientific investigation.
Key Contributions and Concepts:
- Concept of Homeostasis: Bernard's most significant contribution to physiology was his introduction of the concept of the "internal environment" (milieu intérieur) of the body. He proposed that the stability of this internal environment is essential for the maintenance of life, and that all the vital mechanisms of the body, however varied, have only one objective: to maintain the constancy of the internal environment. This idea later evolved into the concept of homeostasis, a fundamental principle in physiology.
- Experimental Methodology: Bernard is also famous for his rigorous approach to scientific experimentation and research. He advocated for the use of the scientific method in physiological studies, emphasizing the importance of hypothesis, observation, and experimentation. His approach significantly advanced the study of physiology and the biological sciences.
- Studies on the Digestive System: Bernard conducted extensive research on the digestive system, discovering the role of the pancreas in digestion and the liver's function in sugar metabolism. He was one of the first to describe the process of glycogen storage in the liver.
- An Introduction to the Study of Experimental Medicine: In 1865, Bernard published "An Introduction to the Study of Experimental Medicine," a seminal work in which he outlined his views on the scientific method in biology and medicine. This book had a profound influence on the development of scientific methodology.
- Ethics in Animal Experimentation: While Bernard conducted animal experiments, he also contributed to the discourse on the ethics of animal testing. His work prompted discussions on the moral implications of using animals in scientific research.
Claude Bernard's contributions have had a lasting impact on the fields of medicine and physiology. His methodological approach and insights into the functioning of the body's internal environment have been fundamental to the development of modern medical science.
13. Antoine Béchamp (1816-1908) was a French scientist whose work spanned multiple disciplines, including chemistry, biology, and pharmacy. He is less well-known than some of his contemporaries like Louis Pasteur, but his contributions to science, particularly in the late 19th century, were significant in several areas.
Key Contributions and Controversial Theories:
- Pleomorphism Theory: Béchamp was a proponent of the concept of pleomorphism, the idea that bacteria can change form (morphology) in response to their environment. This contrasted with the more widely accepted theory of monomorphism, which states that each bacterial species has a fixed shape.
- Microzymas: Béchamp's most controversial theory was his belief in 'microzymas' – tiny particles he believed were the basic form of life and could survive in a dormant state in conditions that would kill other organisms. He theorized that these microzymas were involved in both the creation of cells and in pathological conditions like disease.
- Challenge to Germ Theory: Béchamp's ideas were often at odds with those of Louis Pasteur. While Pasteur is famous for the germ theory of disease, which posits that specific diseases are caused by specific microorganisms, Béchamp believed that the health of the host's body (the "terrain") was more important in determining disease development.
- Chemistry Contributions: Apart from his work in biology, Béchamp made significant contributions to chemistry. He was one of the first to note the presence of an enzyme in yeast and helped in understanding the process of fermentation.
- Influence on Alternative Medicine: Béchamp's ideas have been influential in alternative medicine circles. His emphasis on the internal environment of the body and the conditions that allow pathogens to cause disease has resonated with practitioners who focus on holistic and natural approaches to health.
His emphasis on the internal environment of the body and its role in health and disease continues to influence certain areas of alternative medicine.
14. Arthur Firstenberg is an American author and activist known for his work and advocacy related to the health impacts of electromagnetic radiation.
Key Points:
- Book "The Invisible Rainbow": Firstenberg is best known for his book "The Invisible Rainbow: A History of Electricity and Life," which explores how electricity and electromagnetic fields have been major environmental factors impacting health throughout the 20th and 21st centuries. In the book, he links the proliferation of electrical technology with various health issues, including pandemics.
- Views on Electromagnetic Radiation: Firstenberg argues that electromagnetic radiation from power lines, Wi-Fi, cell phones, and other sources of EMFs pose significant risks to human health and the environment. He asserts that this radiation contributes to a variety of health problems, including chronic diseases and other medical conditions.
- Advocacy and Activism: Firstenberg has been active in campaigning against the expansion of wireless technology, including 5G networks, due to his concerns about their health impacts. He has been involved in various groups and movements advocating for stricter regulation of EMF-emitting technologies.
15. Rudolf Steiner (1861-1925) was an Austrian philosopher, social reformer, architect, and esotericist. He is best known as the founder of anthroposophy, a spiritual movement that posits the existence of an objective, intellectually comprehensible spiritual world accessible to human experience through inner development. Steiner's work and ideas had a profound impact on various fields, including education, agriculture, medicine, and the arts.
Key Contributions:
- Anthroposophy: Steiner's core philosophy, anthroposophy, integrates the spiritual with the scientific. His approach was holistic, focusing on the development of human creativity, freedom, and individuality. Anthroposophy aims to extend the scientific method to include inner experiences as well as external observations.
- Waldorf Education: Steiner is perhaps best known for founding the Waldorf School movement, an educational approach that emphasizes the role of imagination in learning and aims to develop pupils' intellectual, artistic, and practical skills in an integrated and holistic manner. Waldorf schools are known for their focus on creativity, spirituality, and individuality.
- Biodynamic Agriculture: Steiner also pioneered biodynamic agriculture, a method of farming that emphasizes spiritual and cosmic perspectives, including the influence of lunar and astrological cycles. Biodynamics predates the organic farming movement and includes unique practices such as herbal and mineral additives for compost and soil.
- Anthroposophical Medicine: In the realm of medicine, Steiner introduced a holistic approach that combined spiritual insight with practical treatment. Anthroposophical medicine uses a variety of therapies, including diet, exercise, massage, and medications made from natural substances.
- Philosophy and Spirituality: Steiner wrote extensively on a wide range of subjects, including philosophy, the arts, sociology, and spirituality. His works include "The Philosophy of Freedom," which explores concepts of free will and human creativity.
- Architecture and the Arts: Steiner also made contributions to architecture, designing several buildings, including the Goetheanum in Switzerland, the headquarters of the Anthroposophical Society. His influence extends to drama, sculpture, painting, and movement arts (Eurythmy).
Rudolf Steiner's legacy is broad and diverse, influencing thousands of Waldorf schools worldwide, numerous biodynamic farms, and various cultural and artistic institutions. His influence on alternative education, agriculture, and holistic medicine remains significant.
26 Jan 2024 | 3:53 pm
ViroLIEgy 101: Koch’s Postulates
I am starting a series of posts under the heading ViroLIEgy 101 in order to provide relatively short (by my standards) and concise explanations of key concepts regarding both germ "theory" and virology. I'm providing an overview on topics that are essential to the conversation that people may be confused with and have difficulty understanding, or areas that seem to be controversial when engaging in discussions with those defending the germ "theory" of disease.
In this inaugural edition of ViroLIEgy 101, I am focusing on Koch's Postulates as they remain a sticking point for many. These criteria, developed and popularized by German bacteriologist Robert Koch during the late 1800s, are largely considered necessary to satisfy in order to prove that any microbe can cause disease. However, depending on who is asked or what source one turns to, there are ways in which those defending the germ "theory" have attempted to bypass these postulates using various excuses, such as claiming that the postulates are old and outdated, or that they refer only to bacteria rather than "viruses." Let's take a closer look at these postulates in order to see why they are just as relevant and essential today as they were when Robert Koch originally proposed them.

According to Merriam-Webster, a postulate is defined as a hypothesis that is advanced as an essential presupposition, condition, or premise of a train of reasoning. Taking this a step further, it is a logical statement that is assumed true so that a conclusion can be drawn. Postulates do not require any proof as what they state is obvious and stems from common sense.
At the time that German bacteriologist Robert Koch began devising his own logic-based postulates in the late 1870s that would eventually go on to become the standard by which to prove a microbe causes a disease, different aspects of these same logical requirements already existed. In some instances, Koch's Postulates are referred to as the Henle-Koch Postulates as a version of these same criteria had already been proposed by Koch's teacher, German pathologist Friedrich Gustav Jacob Henle. Koch would later modify and go on to popularize them. Henle was one of the early adopters of the unpopular idea that microbes caused disease, stating in his 1840 paper "Von den Miasmen und Contagien und von den miasmatisch-contagiösen Krankheiten" that the "material of contagions is not only an organic but a living one and is indeed endowed with a life of its own, which is, in relation to the diseased body, a parasitic organism." According to Koch's Postulates in Relation to the Work of Jacob Henle and Edwin Klebs, it is said that Henle knew that just finding an organism in a diseased host was not enough to prove causation. The only way to prove the "contagious" nature was to isolate (i.e. separate one thing from everything else) the microbe from the fluids and study it independently. However, Henle felt that this was an impossibility.
"In a discussion published in 1840, Jacob Henle, who was also a pathological anatomist, proposed a criterion for identifying external disease causes. This criterion conformed perfectly with the general strategy that Virchow subsequently discussed. Henle conjectured that many diseases may be caused by parasitic micro-organisms. However, he noted that even if one regularly found living organisms in contagious fluids within diseased bodies, one could still not infer that the organisms were more than harmless saprophytes. The contagion could still be the fluids themselves rather than the organisms. According to Henle, "one could prove empirically that [the organisms] were really effective only if one could isolate…the contagious organisms from the contagious fluids, and then observe the powers of each separately." Henle was sceptical about the possibility of carrying out such a proof, and apparently he never tried to do so."
In addition to Henle's influence on Koch, it is stated that Edwin Klebs, a disciple of the father of modern pathology Rudolf Virchow (ironically, a disbeliever in germ theory), had set forth similar criteria in the early 1870s. Klebs noted that a microbe must be isolated to induce other cases of "infection" and then be observed acting upon the host. He felt that one could infer a causal relationship if different pathological processes, such as inflammation, were noted. As his papers were widely known and discussed, and Koch regularly cited Klebs work, it is argued that Koch was influenced by Klebs own logic-based approach.
In his 1872 paper, Klebs observed that "tracing the invasion and the course of the micro-organisms can make causality probable, but the crucial experiment is to isolate the efficient cause and allow it to operate on the organism." In 1875, he observed that if one could show that "inflammation and other reactive changes follow, step by step, the spread of the schistomycetes, then it is logical to infer a causal relation rather than a simple coincidence." Klebs pointed out that experimental evidence could support the same conclusion. To obtain such evidence, one must "isolate substances from the body and use them to induce further cases of infection." Klebs claimed to have followed both approaches and to have obtained mutually supporting results. His papers and his procedures for establishing causality were widely known and discussed."

If we contrast Edwin Klebs own postulates with Robert Koch's, we can see that the steps that Klebs outlined are very similar to what Koch proposed in 1890 while speaking to the Tenth International Congress of Medicine in Berlin. They both dealt with observation, isolation, and experimentation.
Edwin Klebs Postulates 1877- Anatomical investigations of diseased organs
- The isolation and cultivation of disease germs
- The initiation of new cases of the same disease by conveying germs to healthy animals
- The parasite occurs in every case of the disease in question, and under circumstances which can account for the pathological changes and clinical course of the disease
- After being fully isolated from the body and repeatedly grown in pure culture, can induce the disease anew
- It occurs in no other disease as a fortuitous and nonpathogenic parasite
While there are slightly different ways of stating the criteria that make up Koch's Postulates, there is a commonality in all of them, and typically a fourth postulate, added by plant biologist E. F. Smith in 1905, is presented along with Koch's original three criteria. Thus, Koch's Postulates are regularly written as follows:
Koch's Postulates- The microorganism must be found in abundance in all cases of those suffering from the disease, but should not be found in healthy subjects.
- The microorganism must be isolated from a diseased subject and grown in pure culture.
- The cultured microorganism should cause the exact same disease when introduced into a healthy subject.
- The microorganism must be reisolated from the inoculated, diseased experimental host and identified as being identical to the original specific causative agent.
When going through each of the postulates, it is clear that they are logic-based and rely on common sense. As stipulated by the first postulate, it is logical to assume that, if a microbe were to cause disease, it should only be found in those with the disease while not found in those who are without disease. The presumed pathogen should also not be absent in cases of the disease or found in cases of different diseases. With the second postulate, it is reasonable to require that, when experimenting with an assumed pathogen, one is working with nothing but the pathogen in question in order to rule out contaminants and confounding variables that may influence the results. As for the third postulate, insisting that the same exact disease is established when a healthy host is subjected to a pure source of the presumed pathogen is entirely rational and should be the expected outcome. If no disease is produced or different symptoms are observed, then the presumed pathogen can hardly be the cause of the specific disease being investigated. Finally, it is sound reasoning to require that, if a healthy host does come down with the same disease, the same presumed pathogen should be able to be isolated from the newly sickened host. If it is not, then this would show that the presumed pathogen was not necessary to cause disease and that the experimental procedure or some other confounding variable was likely to blame.
While being entirely logical, the postulates also lend themselves to the concept of falsifiability, which means that they offer a way to disprove that a microbe causes disease. As the postulates are logical and assumed true, anything that goes against them would be considered false. For example, the stipulation highlighted in bold above in the first postulate states that the disease-causing agent "should not be found in healthy subjects." This means that if a microbe that is assumed to be pathogenic is found in healthy hosts, it is falsified as a pathogen as it is found not causing disease. Sometimes, this stipulation is left out of the postulates due to the concept of asymptomatic carriers. However, the very idea of an asymptomatic carrier goes against logic and creates an unfalsifiable concept where the assumed pathogen is able to be found in both the sick and the healthy. There is no way to disprove a microbe as a pathogen if it is found both causing disease and not causing disease. Koch himself denied that bacteria can ever be found in healthy tissues and stated in 1890 that the microbe should not be found in a nonpathogenic form. Thus, even though he did not always practice what he preached, Koch understood the importance of falsifiability and the logic behind the requirements.


Due to their scientific nature, Koch's Postulates serve as a valuable common sense complement to the steps of the scientific method. In fact, they closely align with the scientific method, as noted by virologist Peter Duesberg who stated that they "are science or at least a scientific method." Koch's logical criteria are based upon observation and experimentation, and they crossover with the steps of the scientific method in a few other ways as well. As already discussed, falsifiablity, i.e. the capacity to be shown to be wrong is built into each postulate (sick or healthy, pure or impure, ablity or inability to recreate disease or isolate the same microbe). In order to satisfy the postulates, it is required to identify the causative agent in order to be used as an independent variable prior to experimentation so that it can be determined if it is responsible for producing the disease. Reproducibility is also required to ensure the accuracy of the results. These are all core tenets of the scientific method.

Koch's logical and experimental methods are designed to be used in order to prove a cause-and-effect relationship between a specific microbe and a specific disease. They serve as the overall guide to experimental design as well as a test for the validity of the conclusions, as stated in a 1979 editorial in the American Review of Respiratory Disease.
"Robert Koch, described a logical and experimental process that could be used to prove (by systematic elimination of alternative possibilities) a cause-and-effect relationship between a specific micro-organism and a specific disease. His ideas have been condensed into an elegantly simple and concise set of principles, commonly known as Koch's postulates, which have served the discipline of bacteriology both as an over-all guide to experimental design and as a test of the validity of conclusions."
For two centuries, Koch's Postulates have stood as the "gold standard" for establishing the microbiological etiology of "infectious" disease. They are considered so essential that, according to a 2015 paper by Ross and Woodyard, the postulates are "mentioned in nearly all beginning microbiology textbooks" and "continue to be viewed as an important standard for establishing causal relationships in biomedicine." Lester S. King, a Harvard educated medical doctor who authored many books on the history and philosophy of medicine, wrote in his 1952 paper Dr. Koch's Postulates that Koch's contribution was in "forging a chain of evidence which connected a specific bacterium and a given disease." King stated that this chain was so strong and so convincing "that his principles have been exalted as "postulates" and considered a model for all future work." The Robert Koch Institute stated that Koch's success was due to "the precision with which he developed and applied his scientific methods as well as his logical construction of the chain of evidence."
However, even though the postulates are logical, align with aspects of the scientific method, and are accepted as the "gold standard" causation criteria, there have been many attempts to dismiss them as being nonessential in proving a microbe causes disease. During the "Covid-19 pandemic," various "fact check" articles came out seeking to minimize and disparage the use of Koch's Postulates, such as this article by Reuters published in March of 2021. It attempted to rationalize Robert Koch's bending of his own logical criteria in order to claim that it is acceptable to disregard them altogether. It is true that it was realized early on by Koch and his contemporaries that these logical rules could not be satisfied. Koch himself found the tuberculosis and cholera bacteria in healthy individuals, thus failing his first postulate. For his experiments with anthrax, Koch utilized impure cultures that he claimed were "pure" simply because he found no evidence of contamination when he examined the cultures with a microscope as he had no technique at the time that ensured purity, thus failing his second postulate. He was unable to recreate the cholera disease experimentally utilizing pure cultures of the comma bacillus in animals and even in himself, thus failing his third postulate.

In the paper "The Germ Theory of Disease," Dr. Herbert Snow pointed out that "not a solitary germ yet discovered has succeeded in fulfilling all these conditions" and that "no single microbe put forward by bacteriologists as the cause of a disease has yet complied with more than one." According to the textbook Infectious Diseases (Fourth Edition), the evidence that was gathered by Koch and his contemporaries could not be "fit" to the postulates, and as more and more evidence was acquired, it became rather clear that fulfilling Koch's Postulates was implausible.
"It became apparent almost immediately that there were instances where causation was very likely but the postulates could not be made to 'fit' the evidence. Koch himself believed Vibrio cholerae to be the cause of cholera, but because the organism had also been isolated from otherwise healthy carriers his second principle was breached. As time passed, more and more examples emerged that stretched the utility of Koch's postulates right up to – and indeed beyond – the limit of plausibility."
In fact, it was due to the inability to actually fulfill Koch's Postulates when looking for a bacterial cause of a disease that the very concept of the "virus" was born, as noted by Fields Virology.
"These studies formalized some of Jacob Henle's original ideas in what are now termed Koch's postulates for defining whether an organism was indeed the causative agent of a disease. These postulates state that (a) the organism must be regularly found in the lesions of the disease, (b) the organism must be isolated in pure culture, (c) inoculation of such a pure culture of organisms into a host should initiate the disease, and (d) the organism must be recovered once again from the lesions of the host. By the end of the 19th century, these concepts became the dominant paradigm of medical microbiology. They outlined an experimental method to be used in all situations. It was only when these rules broke down and failed to yield a causative agent that the concept of a virus was born."
As the inability to satisfy the postulates showed that microbes do not cause disease, germ "theory" defenders have tried to disregard the postulates by claiming that they are outdated, too strict, and are no longer necessary. They claim that we now know that asymptomatic "infections" occur, that "viruses" and some bacteria cannot be grown in pure culture, and that human experimentation is unethical, and animals can not be "infected" with certain microbes. The Reuters article claimed that the postulates were devised at a time "when germ theory was still controversial and before the discovery of viruses" which means that Koch's Postulates, as originally written, are outdated and no longer apply. Thus, "modern criteria" such as those proposed by Thomas Rivers and Austin Bradford Hill, which are not Koch's Postulates, are accepted in its place.
However, these excuses put forth to try and explain away the postulates only reinforces that the postulates, as originally devised by Robert Koch, absolutely worked as intended. By failing to satisfy the logic-based rules, microbes as the cause of disease was scientifically disproven. Thus, researchers and "fact checkers" have been trying to either dismiss, work around, or completely revise the postulates (i.e. logic) in a "modern" context in order to continue to try and "fit" the evidence to make the germ "theory" of disease work. Being unable to falsify the hypotheses and being unwilling to change in the face of contradictory evidence are the very hallmarks of pseudoscience.

Regardless of the excuses, the main "infectious" disease institutions in the world still maintain that Koch's Postulates, as originally devised, must be satisfied in order to prove that any microbe, including "viruses," are the cause of a disease. For instance, the WHO stated, during the original "SARS epidemic" in 2003, that all of Koch's Postulates must be satisfied:
"Conclusive identification of a causative must meet all criteria in the so-called "Koch's postulate." The additional experiments needed to fulfil these criteria are currently under way at a laboratory in the Netherlands."
https://web.archive.org/web/20210105005624/https://www.who.int/csr/don/2003_03_27b/en/
On April 16th, 2003, the WHO outlined exactly what steps are required in order to prove a microbe causes disease:
"The 13 laboratories have been working on meeting Koch's postulates, necessary to prove disease causation. These postulates stipulate that to be the causal agent, a pathogen must meet four conditions: it must be found in all cases of the disease, it must be isolated from the host and grown in pure culture, it must reproduce the original disease when introduced into a susceptible host, and it must be found in the experimental host so infected."
As can be seen, these are Koch's original postulates. These are not the revised "modern" versions supplied by Thomas Rivers, Austin Bradford Hill, or anyone else for that matter. In agreement with the WHO on the importance of Koch's Postulates, the CDC's own field manual published in 2018 titled Optimizing Epidemiology–Laboratory Collaborations, stated that Koch's postulates form the basis of proof that an emerging agent is the etiological cause of a disease. Each of the postulates was considered necessary to satisfy as just finding an agent does not mean that it is the cause of disease:
"In field investigations that involve emerging pathogens, Koch's postulates form the basis of proof that an emergent agent is the etiologic agent. Therefore, the interpretation should consider the successful fulfillment of each of Koch's postulates. Just because an agent is found does not necessarily mean it caused the disease."
https://www.cdc.gov/eis/field-epi-manual/chapters/Epi-lab-Collaboration.html
Various virologists have also agreed with both the WHO and the CDC that fulfilling Koch's Postulates is necessary. In 2012, Zaki et al. stated that Koch's Postulates were important to determining if their "virus" was the causative agent of severe respiratory disease:
"Epidemiologic investigations, active case findings with the use of updated case definitions, and syndrome surveillance in combination with sensitive diagnostic tests will be key to monitoring the present situation and — if necessary — to intervene in a potential outbreak. It will be equally important to test whether HCoV-EMC fulfills Koch's postulates as the causative agent of severe respiratory disease."
Zaki MERS "Coronavirus" Paper (2012)

This was backed up by virologist Ron Fouchier, the lead researcher for the 2003 "SARS" paper claiming fulfillment of Koch's Postulates, who stated (wrongly) that it was KOCH'S Postulates that were fulfilled for "SARS" while speaking about the need to once again fulfill them for MERS:
Ron Fouchier on the New Coronavirus: We Need to Fulfill Koch's Postulates"For starters, we'll find out whether animals get sick from this virus. You can isolate a virus from a patient, but that does not mean they died from it; to show that it causes disease you need to fulfill Koch's postulates. That's what we did for SARS, and it's what we hope to do here; we've applied for emergency ethical approval."
This was echoed by researchers in 2020 when discussing the fact that "SARS-COV-2" had not fulfilled Koch's Postulates. According to Zhou et al., the experiments to fulfill the postulates had not been carried out:
"However, there are still many urgent questions that remain to be answered. The association between 2019-nCoV and the disease has not been verified by animal experiments to fulfil the Koch's postulates to establish a causative relationship between a microorganism and a disease. We do not yet know the transmission routine of this virus among hosts."
Zhou "SARS-COV-2" Paper (2020)
This same sentiment was reiterated by Zhu et al. who admitted that they had not fulfilled Koch's Postulates and that these experiments remained to be completed:
"Although our study does not fulfill Koch's postulates, our analyses provide evidence implicating 2019-nCoV in the Wuhan outbreak. Additional evidence to confirm the etiologic significance of 2019-nCoV in the Wuhan outbreak include identification of a 2019-nCoV antigen in the lung tissue of patients by immunohistochemical analysis, detection of IgM and IgG antiviral antibodies in the serum samples from a patient at two time points to demonstrate seroconversion, and animal (monkey) experiments to provide evidence of pathogenicity."
Zhu "SARS-COV-2" Paper (2020)
In chapter one of the fifth edition of Plant Pathology, it is stated that Koch's rules are, in fact, possible to implement with all "pathogenic" microbes, even though they are not always easy to carry out. However, it states that in the cases where culture or purification of the pathogen is not yet possible and the pathogen cannot be reintroduced to produce the disease, Koch's Postulates cannot be carried out. Thus, the acceptance of these microbes as the actual causes of the diseases they are associated with is considered tentative, and it is assumed that further improvement of techniques of isolation, culture, and inoculation of pathogens will someday prove that these assumptions are justified.
"Koch's rules are possible to implement, although not always easy to carry out, with such pathogens as fungi, bacteria, parasitic higher plants, nematodes, most viruses and viroids, and the spiroplasmas. These organisms can be isolated and cultured, or can be purified, and they can then be introduced into the plant to see if they cause the disease. With the other pathogens, however, such as some viruses, phytoplasmas, fastidious phloem-inhabiting bacteria, protozoa, and even some plant pathogenic fungi that are obligate parasites of plants (such as the powdery mildew, downy mildew, and rust fungi), culture or purification of the pathogen is not yet possible and the pathogen often cannot be reintroduced into the plant to reproduce the disease. Thus, with these pathogens, Koch's rules cannot be carried out, and their acceptance as the actual pathogens of the diseases with which they are associated is more or less tentative. In most cases, however, the circumstantial evidence is overwhelming, and it is assumed that further improvement of techniques of isolation, culture, and inoculation of pathogens will someday prove that today's assumptions are justified."

It is clear to see that, contrary to what the defenders of the germ "theory" want you to believe, Koch's Postulates are still relevant today and fulfilling all of the postulates is considered necessary in order to prove any microbe can cause disease. Without fulfilling Koch's logical rules, the "pathogenic" designation is tentative and awaits to be proven in the future. The defenders of germ "theory" do not want to accept this as they know full well that no bacterium has satisfied all four steps of Koch's Postulates. They also know that, as stated by virologist Thomas Rivers, "it is obvious that Koch's Postulates have not been satisfied in viral diseases." Thus, they want you to believe that the postulates are outdated and do not pertain to "viruses." However, the postulates apply to all microbes and are not outdated. This was summed up brilliantly by virologist Peter Duesberg when he was questioned whether Koch's criteria are outdated and unable to be used to establish HIV as the cause of AIDS:
"Koch's postulates are pure logic. Logic will never be "out of date" in science."
-Peter Duesberg
This article originally appeared on ViroLIEgy's Antiviral Substack.
19 Jan 2024 | 1:37 pm
The Infectious Myth Busted Part 6: The Germ Duel
In the early 1900s, there was a Canadian doctor who experimented with millions of the so-called deadly pathogenic bacteria of diphtheria, typhoid, pneumonia, meningitis, and tuberculosis. Anywhere from 50,000 to several millions of these bacteria were contained within the cultures that were ultimately swallowed by the volunteers. However, not a single one of them ever came down with disease over the course of the five years of experimentation. Having satisfied himself of the fraud of the germ "theory" of disease, the Canadian doctor set out a challenge to the rest of the scientific community to prove that microbes can cause disease through similar experiments. While his challenge was largely ignored, a doctor from Minnesota eventually responded by issuing a challenge of his own to the Canadian doctor, wanting him to subject himself to further experiments. Thus, a germ duel was set where the person with the positive claim regarding the existence of so-called deadly pathogenic microbes wanted the one who challenged this belief to prove it wrong by experimenting directly on himself.
Often times when dealing with the defenders of the germ "theory" of disease, we are challenged to similar "germ duels" where, in order to maintain our honor and support our challenge to their positive claim (which they mistakenly believe has been satisfied due to a hundred years of pseudoscientific experimentation), we must demonstrate a willingness to "risk our lives" for it while they get to sit back on fraudulent evidence that they feel is sufficient. We are supposed to subject ourselves to various so-called "pathogenic" agents in order to disprove "infection" and "contagion." This is a defensive tactic that is employed once the germ "theory" defenders realize that they have no scientific evidence on their side supporting their belief in invisible "pathogenic" boogeymen. Thus, it somehow becomes "logical" in their minds to demand that we jump through ridiculous hoops in order to satisfy their outlandish scenarios in place of their having to provide experimental evidence that validates the positive claims that they make. It's an attempt to logically fallaciously shift the burden of proof onto us so that they do not have to defend their position with scientific evidence. Personally, I've been told to get bit by a rabid dog, sleep with someone who has an STD, inject myself with HIV-positive blood, sit inside a tuberculosis ward, and take care of an Ebola patient without adequate protection.
Ironically, I can actually cross one of those scenarios off of the list as I personally lived inside a small two-bedroom apartment with my mother-in-law who was said to be in the active and "infectious" phase of the tuberculosis disease for over a month. According to the Mayo Clinic, TB spreads when a person ill with the disease coughs, sneezes or sings, releasing tiny droplets with the germs into the air that another person breathes in, allowing the germs to enter the lungs. The disease is said to spread easily when people gather in crowds or when living in crowded conditions. However, despite the fact that it should have been easy for us to "catch" the disease, neither myself, my wife, my son, nor any of the various relatives and visitors who came to see my mother-in-law during that time ever came down with the tuberculosis disease or even tested positive for it. This was a major turning point that had me questioning the concepts of "infectiousness" and "contagiousness."
While I may not personally be able to cross the other challenges regularly issued to me off of the list, these kinds of scenarios and experiments have been done before. Take, for instance, when Dr. Robert Wilner injected himself with the blood of an HIV positive patient on live TV (starts at around the 40-minute mark). Dr. Wilner remained fine, never testing positive for HIV or developing AIDS. He eventually died of a heart attack.
As far as sleeping with someone with an STD, while investigating whether or not one can "catch HIV" from an "infected" partner, Nancy Padian's 1996 study followed 175 discordant couples (1 HIV positive and the other negative) for 10 years. These couples regularly slept together and had unprotected sex. There were no HIV transmissions from the positive partner to the negative partner during the entirety of the study:
Heterosexual Transmission of Human Immunodeficiency Virus (HIV) in Northern California: Results from a Ten-year Study"We followed 175 HIV-discordant couples over time, for a total of approximately 282 couple-years of follow-up (table 3). Because of deaths as well as the break-up of couples, attrition was severe; only 175 couples are represented in table 3. The longest duration of follow-up was 12 visits (6 years). We observed no seroconversions after entry into the study."
"At last follow-up, couples were much more likely to be abstinent or to use condoms consistently, and were much less likely to practice anal intercourse (p < 0.0005 for all). Nevertheless, only 75 percent reported consistent condom use in the 6 months prior to their final follow-up visit. Forty-seven couples who remained in follow-up for 3 months to 6 years used condoms intermittently, and no seroconversions occurred among exposed partners."
"In general, we estimate that infectivity for male-to-female transmission is low, approximately 0.0009 per contact, and that infectivity for female-to-male transmission is even lower."
"While lack of transmission in our prospective study may in part be due to such unidentified protective
factors, we also observed significant behavior change over time. In previous reports (8, 14, 29), the proportion of couples who used condoms at their last follow-up prior to analysis was 100 percent; the 75 percent reported here is the lowest proportion that we have observed. The proportion of couples who would use condoms if the study were continued beyond 10 years remains unknown. Nevertheless, the absence of seroincident infection over the course of the study cannot be entirely attributed to significant behavior change. No transmission occurred among the 25 percent of couples who did not use condoms consistently at their last follow-up nor among the 47 couples who intermittently practiced unsafe sex during the entire duration of follow-up. This evidence also argues for low infectivity in the absence of either needle sharing and/or cofactors such as concurrent STDs."
With regard to being bitten by a rabid dog, according to leading Louis Pasteur researcher Gerald Geison, there is a very high degree of uncertainty in the correlation between animal bites and the subsequent appearance of rabies-even when the biting animal is certifiably rabid. He also stated that most victims of rabid animal bites could forego treatment without experiencing disease in the future. These statements are backed up by a report by physician and surgeon Millicent Morden titled Rabies Past Present in Scientific Review, wherein it is reported that many instances of bites by rabid dogs over many decades resulted in zero cases of rabies amongst those who were bitten, and the vaccine itself was to blame for so-called rabies deaths:
"Dr. Matthew Woods, another contemporary of Pasteur, then a leading member of the Philadelphia Medical. Society, wrote much on the subject of rabies. He stated, "at the Philadelphia dog pound, where on an average more than 6,000 vagrant dogs are taken annually, and where the catchers and keepers are frequently bitten while handling them, not one case of hydrophobia has occurred during it's entire history of twenty-five years, in which time 150,000 dogs have been handled."
"The records of the London Hospital, a few years ago, showed 2,668 persons bitten by angry dogs. None of them developed hydrophobia."
St. George's Hospital, London, records 4,000 patients bitten by dogs supposed to have been mad. No case of hydrophobia.
Dr. Dulles, previously referred to, has said, "I might cite my own experience in the treatment of persons bitten by dogs supposed to be mad, which has furnished not a single case of the developed disease in thirty years. And I have probably seen more cases of so-called hydrophobia than any other medical man." Dr. Dulles was lecturer on the History of Medicine at the University of Pennsylvania, Consulting Surgeon to Rush Hospital and Manager of University Hospital."
"There are over 3,000 deaths on record in reports from the Pasteur Institute, of persons bitten by dogs. All died after treatments. On the other hand, the record of the London Hospital, a few years ago, showed 2,668 persons bitten by angry dogs: not one of them developed hydrophobia and not one had been treated by the Pasteur method."
In the case of being exposed to Ebola, a researcher accidentally injected herself with the "deadly" Ebola "virus" during an outbreak in 2009. While she was said to be "saved" from experiencing the disease due to an experimental vaccine she received that was never before tried on humans, the case can easily be made that she was in no danger at all of ever developing disease even had she never taken the experimental injection. In 2014, a woman took care of 4 family members without using adequate personal protective equipment, relying instead on a raincoat and trash bags, and never contracted the disease. In another example, researchers of a 2016 study on an Ebola outbreak hotspot in Sierra Leone used antibody testing on 187 participants who had been previously quarantined due to sharing a public latrine with a confirmed case or based on a confirmed case living with them. Of the 187 who had direct contact with Ebola patients, 14 were said to have been "infected" at some point in time, even though 12 reported no symptoms whatsoever, while the other 2 reported remembering only having a fever at the time. In other words, despite what the fraudulent antibody results showed, none of the 187 who had direct contact with Ebola patients actually became sick with the disease, even while living with them:
Ebola Might Not Make Some People Sick, Study Finds In at least one village in Sierra Leone, it seems that up to a quarter of those infected may never have known it."Our data indicate that 25 percent of Ebola virus infections may have been minimally symptomatic," an international team of researchers writes in the Public Library of Science journal PLoS Neglected Tropical Diseases."
"They chose the village of Sukudu in the diamond-rich Kono District. Richardson had been working there with the charity Partners in Health. The collected blood from 187 people who had been quarantined after they shared latrines with known Ebola patients.
They found 14 with antibodies to Ebola, something that suggested they'd been infected. Twelve of the 14 said they did not remember ever having had a fever or being sick during that time."
Health workers had kept a close eye on villagers, so the researchers believe it's unlikely the people hid their illness.
"Our data suggest that a significant portion of Ebola transmission events may have gone undetected during the epidemic," the team wrote.
https://www.google.com/amp/s/www.nbcnews.com/news/amp/ncna684431
These are but a few examples of instances where people were exposed, either deliberately or unknowingly, to so-called "pathogenic" microbes and the expected disease did not occur. This evidence should be enough to show that the germ duel challenge that is regularly proposed by the germ "theory" supporters as a defensive mechanism is dead-on-arrival. No matter how many pseudoscientific studies they throw out in an attempt to support their position, there is plenty of evidence that contradicts and completely demolishes any claims of "infectivity" and "contagiousness." However, in honor of the proposed germ duel between the doctors of the north from Canada and Minnesota in the early 1900s, I want to share many other instances throughout the formulative years of the germ "theory" of disease where people exposed themselves (and others) to so-called pathogenic microbes in natural ways. Some did so with the intention of showcasing the fraud of the germ "theory" of disease. Others were attempting to prove it or use it to their advantage. What will be clear after examining these additional cases is that, even though the germ "theory" duelists are the ones issuing the challenge, we have all of the ammo, and they have nothing but blanks to shoot in return.

This first instance of self-experimentation was of the accidental variety as presented from The Germ Theory of Disease by Dr. Herbert Snow. It is stated that, upon testifying in front of a jury, Dr. John Thresh related a story about his accidentally drinking a pure culture of typhoid bacillus. He remained completely fine without any ill health effects.
"Dr. Thresh, the well-known Medical Officer of Health, told the jury in the Malvern Hydro Citse, that be had accidentally swallowed a wineglassful of the "pure culture" of virulent typhoid bacilli without the smallest ill-consequence."
From the same source, it is shared that Dr. Emmanuel Edward Klein did not believe that Robert Koch had actually discovered the true cause of cholera. In order to prove this, he drank a wineglassful of a pure culture of comma bacilli without experiencing any ill effect:
"Dr. Klein, who was about to proceed to India to investigate the origin of that disease, did not believe in Professor Koch's statement and experimentally drank a wine-glassful of comma bacilli in "pure culture." No effect followed; and Dr. Klein remains alive and well to this day."
This account can be verified by the 2010 paper 1885 Cholera Controversy: Klein versus Koch:
"According to Waller, on this occasion Klein made the first microbiological auto-experiment by drinking water infected with comma bacillus to prove its uncontagiousness, which was soon repeated by Max von Pettenkofer."
As noted, Klein's experiment was also performed by Max von Pettenkofer, considered the greatest authority on cholera, and who was another critic of Robert Koch. At the age of 74, he ingested a pure culture of comma bacilli. While he experienced a light diarrhea, it was not considered to be reflective of the cholera disease. Two other students attempted the same, and while they were said to develop a "severe cholerine" (which is defined as mild diarrhea), the experiments ultimately showed that clinical cholera "was certainly not an inevitable consequence of ingesting virulent cholera bacillus."
Pettenkofer Revisited"Pettenkofer was so convinced that the organism alone was insufficient to cause illness that he resolved to carry out the "experimentum crucis" on his own person. This famous event occurred on October 7, 1892 when he was 74 years old. He obtained a fresh culture of cholera vibrio isolated by Prof. Gaffky from a patient dying of cholera. A transfer was made into bouillon and he swallowed 1.0 cc on an empty stomach after neutralizing the acidity with sodium bicarbonate. No symptoms developed except a "light diarrhea with an enormous proliferation of the bacilli in the stool." Of this experiment Pettenkofer wrote:
"Even if I had deceived myself and the experiment endangered my life, I would have looked Death quietly in the eye for mine would have been no foolish or cowardly suicide; I would have died in the service of science like a soldier on the field of honor. Health and life are, as I have so often said, very great earthly goods but not the highest for man. Man, if he will rise above the animals, must sacrifice both life and health for the higher ideals." (from Ref. 1)
I am told by Prof. Eyer, current Professor of Hygiene at Munich, that Pettenkofer undoubtedly had had cholera himself during the epidemic of 1830, so that little immunity probably persisted. (Personal communication at Munich, Aug. 1972). Several of Pettenkofer's students followed their master's example. Two of them were not as lucky (or as immune) so that a severe "cholerine" developed but there were no deaths. These experiments showed that clinical cholera was certainly not an inevitable consequence of ingesting virulent cholera bacillus."

According to the book The Illusion of Viral Contagion_Scientific and Philosophical Review, Dr. Rudolph Emmerich, who was Dr. Pettenkofer's disciple, injected himself with cholera on stage in front of an audience and survived. His experiments with injecting cholera is verified as well in his 1914 New York Times obituary.
"He performed this on a stage in front of an audience of over a hundred people and survived. Emmerich carried out a number of experiments on himself by injecting several strains of cholera bacilli into his body the results of which proved that cholera is less virulent when contracted from a human being in contradistinction to that from drinking contaminated ground water."
https://theillusionofviralcontagion.co.uk/
According to the book Immunity: How Eli Metchnikoff Changed the Face of Modern Medicine, Russian-born zoologist Ilya Metchnikoff and his fellow researchers drank "glass after glass of water mixed with cholera germs from the Seine, from the stools of sick people, from a fountain on one of the squares in Versailles." While one volunteer nearly died, Metchnikoff and another volunteer remained perfectly healthy.
"Which brings us to 1892. A cholera epidemic was sweeping in France, and Metchnikoff was struggling to understand why the disease struck some people and not others. To do so, he sucked down a drink full of cholera. He never got sick, so he let a volunteer drink some as well. When that volunteer failed to get sick as well, Metchnikoff offered the drink to a second test subject. That man, however, didn't fare so well. He got cholera and nearly died."
https://www.smithsonianmag.com/smart-news/thank-man-who-drank-cholera-your-yogurt-180955197/
Ironically, the most damning evidence against the cholera bacillus actually came from Robert Koch himself. After failing to "infect" and reproduce the disease in animals, Koch tried to "infect" himself by drinking pure cultures. Like Pettenkofer, Koch had a mild case of diarrhea that was not reflective of the disease, and the unfavorable result was ultimately used to ridicule him.
In order to fulfill the criteria laid down in the remaining two of his postulates, Koch tried to infect animals with pure cultures of the organism with little success. He rightly concluded that the animals were not susceptible to cholera and took recourse to the extreme step of infecting himself by drinking pure cultures. However, he came down with only a mild episode of diarrhoea, an outcome which was later on exploited by his opponents to ridicule him."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3089047/

While the above examples about the inability to reproduce both typhoid and cholera through the ingestion of pure cultures by various researchers is compelling evidence against the germ "theory" of disease, these next examples are absolutely damning. In 1901, Dr. Matthew Rodermund deliberately subjected himself to a smallpox patient by opening the wounds and smearing the pustules all over his face, hands, beard, and clothes. He then went home to have dinner with his family and returned to his office afterward. He met up with a reverend friend whom he exposed, as well as many patients he saw as he touched their faces with his hands. Dr. Rodermund then went to a Business Men's Club where he played poker with other men, exposing them all. He slept at home with his family and then traveled to Green Bay the next morning by train to eat breakfast and work with 27 patients. He did not wash himself or change his clothes throughout the entire time.
By the next day, reporters had found out about this experiment and asked Dr. Rodermund about the affair. He told them the truth and was eventually quarantined by the police. However, Dr. Rodermund broke quarantine and traveled to Chicago, to Terre Haute, Indiana, and then back home, exposing more people before he was finally arrested. The authorities attempted to trace cases of smallpox to Dr. Rodermund, who, by his own estimate, exposed over 50,000 people throughout his journey, but they were unable to find even a single case of smallpox resulting from the doctors actions to pin on him.
Dr. Rodermund's Experiment"Then to show them that this was true, I broke open several of the large pustules on her face and arms and took the pus out of them and smeared it all over my face, hands, beard and clothes, and at the same time remarked that I would now go home to dinner.
I mentioned nothing of the affair to my family during the meal and went directly to my office without telling anyone."
"The reader can imagine the state of my mind at that time, as none of them had an inkling that I was at that very time covered with smallpox pus, and that the cards we were playing with were being loaded with this poison. Still, I never once mentioned my visit to them. Further, I would never have gone to the club-rooms if I had had the least idea that my actions would ever be known, as I knew the sentiment of these gentlemen and I also had too much respect for them and myself, to impose upon their feelings, even if I did know that their belief was a foolish superstition. I have done similar acts dozens of times during the past fifteen years and have in each instance watched the results and not the slightest harm has ever been done to anyone.
To return to our subject, after leaving the club-rooms that evening I went home, slept with my family, and the next morning took the train to Green Bay, without washing my hands or face, and wearing the same clothes."
"The sanctimonious frauds and deceivers of the public (doctors) tried in every way, shape and manner, to trace a case of smallpox to my actions, but with no avail. Even after I had exposed 50,000 people, and rubbed my pus-covered hands over thirty-seven faces, they could find nothing against me. In the near future I will publish a few similar incidents which have happened to me the past years, and which are far more interesting than this one."
https://archive.org/details/vaccinationsupe00hodggoog/page/n57/mode/1up
Dr. Rodermund later wrote about further experiments that he performed where he attempted to "infect" seventeen people with consumption, scarlet fever, smallpox or diphtheria by spraying the germs into the throat and nose, or having them breathe the germs into the lungs. He repeated these experiments every one or two weeks for months, and none of the subjects became ill.
"I wanted to be so absolutely certain that I was not going to spring a question of so much importance upon the public which could not stand the test and brunt of any investigation that it might be subjected to. I made the experiments upon seventeen people between the ages of fifteen and thirty years, but in no instance could a case of consumption, scarlet fever, smallpox or diphtheria be produced.
These experiments were made in the following manner: I sprayed the poisons of diphtheria, small-pox, scarlet fever, or consumption into the throat, nose, or had them breathe them into the lungs, repeating the experiment in most cases every one or two weeks for months, with the result that no disease could be developed. Of course, I could not let the patients know what I was doing. I was supposed to be treating them for catarrh of the nose or throat."
https://archive.org/details/medicalbrief04unkngoog/page/282/mode/1up
In another instance of self-experimentation, according to a paper from December 1896, it was announced that Dr. Thomas Powell had experimented on himself with all manner of "pathogenic microbes." He was confident in his results and had written various scientific articles about the topic:
A NEW CURE-ALL. A Patent Sanitarium to Be Located in Los Angeles. COLUMBIA. Mo., Dec. 4.—Dr."Thomas Powell of Columbia, claims to have learned hnw to inoculate the human system so as to render it impervious to disease genus. As vaccination prevents smallpox, so this discovery will ward off scarlet fever, consumption, diphtheria, and every other disease caused by germs. So confident is Dr. Powell of the truth of his discovery that he has written largely for scientific journals on the subject and has himself tested it practically by exposing himself to ail manner of diseases. He entered this week into an agreement with California capitalists by which he is to be paid $9000 for a one-third interest in the discovery."
https://www.newspapers.com/article/los-angeles-herald-dr-thomas-powell-s/4831433/

In a Los Angeles Herald article from November 1897, details of Dr. Powells experiments were provided. It was stated that Dr. Powell exposed himself over a period of ten years to the germs of the deadliest diseases in order to shatter the theory of the transmission of contagious disease from one person to another. Dr. Powell not only survived, but he never experienced any ill effects from the undertaking of his experiments. His results were considered conclusive as they were achieved in the presence of two well-known physicians who corroborated the findings. Dr. Powell stated that his experiments proved that germs are the result of, and not the cause of, disease and that they are beneficial to achieving and maintaining health. So convinced was he of his results, Dr. Powell also used family members and other volunteers in his experiments along with himself. He cultured the typhoid, diphtheria, and glanders bacteria to the point of there being no doubt about their "virulent nature," and he experienced no ill effects beyond a sore arm from the injection. Dr. Powell stated that his greatest trial occurred in the presence of 25 physicians where he took both the typhoid and diphtheria bacteria into his system and, upon examination, it was determined that no ill effects had occurred. In order to ensure that there could be no doubters, Dr. Powell performed the same experiments on two patients who also experienced no ill effects. Dr. Powell was confident that the germ "theory" of disease was fraudulent and challenged anyone to bring forth the most "virulent" bacteria so that he could ingest them. The physicians who witnessed these results firsthand were dumbfounded.
DEADLY GERMS How Dr. Thos. Powell Has Swallowed Them BACILLI IN HIS SYSTEM HE LAUGHS AT THE THEORY OF CONTAGION Gives to the World the Story of His Ten Years' Defiance of the Death-Dealing BacilliMen have done strange things and taken desperate chances in the interests of science, but none has been stranger or more desperate that the act ot Dr. Thomas Powell, a physician who about a year ago took up his residence in this city, and who has actually taken into his system during the past ten years the germs of the deadliest diseases, for the specific purpose of shattering the time-honored theories regarding the transmission of contagious complaints from one person to another. Incredible as it may seen, Dr. Powell has not only survived the desperate experiments that he has undertaken, but has never shown the slightest signs of any ill effects resulting from them. The evidence regarding the truth of his claim is conclusive. His own written statements are backed up by the testimony of well-known physicians in whose presence Dr. Powell has taken the germs into his system during experiments that he has been secretly making during the past ten years.
Dr. Powell has decided that the time has come for giving to the world the result of his experiments, which he claims have been a complete and unqualified success. Here is the doctor's statement of the result of his defiance of the power of germs:
"Before going into the details of my experiments with the germs of virulent diseases. I want to preface my statements with the explanation that I do not declare the germs to be harmless in all cases. What I do say is that a person to whom the germs of a particular disease are likely to prove dangerous must have a predisposition towards that particular disease, such predisposition being either hereditory or acquired. Given a man or woman with no such predisposition, and I claim that the deadliest germs are powerless to harm them. They can enter the sick chamber without fear of contracting disease, or even do as I have done, take the living germ into their system and suffer no harm. My experiments have proved the truth of my theory. "I claim that disease germs are utterly incapable of successfully assailing the tissues of the living body; that they are the results and not the cause of disease; that they are not in the least inimical to the life or health of the body; that, on the contrary, it is their peculiar function to rescue the living organism, whether of man or beast, from impending injury or destruction. They'accomplish this by bringing about the decomposition of that obstructing matter which constitutes predisposition to disease, and cause it to be passed out by tlie blood.
"For ten years I have worked on this theory, and the results achieved I now give to the world. I determined in the first place to experiment by inoculating, not an animal whose hold upon life is exceedingly feeble, as is that of the rabbit or guinea pig, but the human body. I made the experiments upon myself, then upon members of my own family, and lastly upon such patients as were within the range of safe experimentation. I inoculated myself with the most virulent typhoid bacilli obtainable, having first eradicated from my system any predisposing cause for the disease. The result was entirely satisfactory, no evil ensuing beyond the usual soreness as in vaccination. Then I took into my system the typhoid bacilli, and no typhoid fever making its appearance, I repeated the experiment with diphtheria germs, without the least perceptible effect.
"In order to make the experiments still more complete, I cultivated the germs of diphtheria and glanders until there could be no doubt of their virility and took them into my system in the presence of two reputable physicians. The outcome was (illegible) the same as before.
"Then I made the greatest trial of all. In the presence of twenty-five physicians I took, first, the bacilli of typhoid into the stomach enclosed in gelatine capsules; and, second, the bacilli of diphtheria by both the vaccination method and subcutaneous inoculation.
"Examinations were afterwards made by the physicians referred to of the pulse, the temperature and of the respiration, and it was unanimously declared that these inoculations produced no greater effect upon me than might have been expected from a like quantity of water.
"In order that there should be no possibIlity of doubting Thomases declaring that the experiments were successful only in my case and that I had in some way been made contagion-proof by nature, I singled out from among my patients two who appeared to be fit subjects for similar experimentation: and, with their consent, put them through the same course as I had undergone, with less virulent diseases. The outcome proved that my calculation were well founded, no evil resulting in their ease any more than in mine.
"I am progressing towards a climax in my opposition to the greatest delusion of the world's history, which will consist of the most astounding and conclusive demonstration ever made in the establishment of a scientific proposition. So confident am I that the scientists of the world are at fault in their germ theories that I challenge anyone to bring to me the bacilli of any disease known to the medical profession, and I promise to take into my system, in the presence of any jury of physicians that may be selected, germs that have been cultivated into deadly activity by ths usual processes. All I ask is that I may be given time to eradicate from my system any predisposition to the disease that the germ represents."
The physicians in whose presence Dr. Powell has made the experiments have been completely dumfounded by the ease and facility with which he has uprooted medical landmarks and smashed the chilled-steel theories of science. While admitting that there is no room for doubting the truth of his statements, they are not willing to admit that the theories can be applied generally.
The matter is of so much importance, however, that they are arranging to have a great and convincing test made by Dr. Powell and anyone who is willing to submit to the same inoculation as he has done, in order to settle forever the great question of whether or not a supposedly contagious disease can be transmitted from one person to the other by the medium of germs. The whole world will await the outcome with interest.
DR. THOMAS POWELL
https://cdnc.ucr.edu/?a=d&d=LAH18971121.2.200&dliv=none&st=1&e=——-en–20–1–txt-txIN——–
Similar experiments to those done by Dr. Powell were carried out by Dr. John B. Fraser, as reported in his article "Do Germs Cause Disease?" published in the Physical Culture Magazine for May 1919. The excerpt below is reprinted from Dr. Herbert Shelton's 1939 book The Hygienic System. In his experiments, Dr. Fraser utilized millions of the highly "virulent" germs of diphtheria, pneumonia, typhoid, meningitis, and tuberculosis and fed them to volunteers in various ways. In all instances in over 150 experiments conducted over a 5-year period, no disease ever occurred in any of the volunteers.
"The first experiment made was taking fifty thousand diphtheria germs in water, and after a few days suspense and no sign of the disease it was considered that the danger had passed.
In the second experiment one hundred and fifty thousand diphtheria germs were used in milk, and again no signs of diphtheria appeared.
In the third experiment over one million diphtheria germs were used in food without producing any sign of the disease.
In the fourth experiment millions of diphtheria germs were swabbed over the tonsils and soft palate, under the tongue, and in the nostrils and still no evidence of the disease was discernible. As these results were very satisfactory it was decided to test out some other kinds of germs. A series of tests were made with pneumonia germs in which millions of germs were used in milk, water, bread, potatoes, meat, etc., and although persistent efforts were made to coax them to develop absolutely no sign of the disease appeared.
Another series of experiments were carried out with typhoid germs, special care being taken to infect distilled water, natural milk (not pasteurized) ; bread, meat, fish, potatoes, etc., etc., with millions of the most vigorous germs that could be incubated, and but for the knowledge that they had been taken, one would have known nothing about it.
Another series of tests were made with the dreaded meningitis germs, and as the germs are believed to develop mainly in the mucous membranes of the nostrils, special pains were taken to swab millions of the germs over the floor and sides of the nostrils, into the turbinated sinuses, over the tonsils, under the tongue, and back of the throat. In addition to these tests other tests were made in food and drink–millions of germs in each case, and yet no trace of the disease appeared. The experiments with the tuberculosis germs were carried out in a different way–more time was given between the experiments so as to allow the germs to develop; for clinical evidence has shown that this disease may remain latent, or imperfectly developed for months. Consequently it meant months of watching and waiting before one could be positive that the germs would not develop.
Here again millions of germs were used in water, milk, and food of various kinds; every variety of food and drink was concerned; and as almost five years have elapsed since the experiment with T.B. began and no evidence of the disease has appeared I think we are justified in the belief that the germs are harmless. In addition to those experiments combinations of germs were used, such as typhoid and pneumonia, meningitis and typhoid, pneumonia and diphtheria, etc., etc., but no evidence of disease followed. During the years 1914-15-16-17-18 over one hundred and fifty experiments were carried out carefully and scientifically and yet absolutely no signs of disease followed."
Dr. Fraser provided further explanation in an article published in The Canada lancet: Vol. 49, no. 10 (June 1916), where he pointed out that bacteria are never found when they should be, which is at the beginning of the disease process. The bacterium follows after the disease has developed. Dr. Fraser highlighted his own experiments ingesting diphtheria, typhoid, and pneumonia bacteria. At no time did any disease develop in Dr. Fraser or any of the subsequent volunteers.


https://www.canadiana.ca/view/oocihm.8_05199_550/15

While Dr. Rodermund, Dr. Powell and Dr. Fraser's experiments are damning in and of themselves, there will be those who may be put off by the results of anyone working with the intention of disproving the germ "theory" of disease. Thus, let's look at an example where a person very badly wanted the germ "theory" of disease to work out, and the fact that it didn't ultimately blew up in his face. In 1916, dental surgeon Arthur Waite married the daughter of a very successful pharmaceutical businessman by the name of John Peck. Wanting to seize Peck's vast fortune for himself, Waite decided to kill John, his wife Hannah, and his sister Catherine. To do so, Waite attempted to poison them with what he thought were deadly germs that he had accessed from laboratory cultures from sources such as the Rockefeller Institute for Medical Research and the Cornell Medical Center. Waite began by trying to poison Peck's sister Catherine when he added the bacteria cultures to her soup. Once he realized that his plan had failed to bring about disease, according to his own testimony, Waite stated that he gave her "repeated doses of germs, then some arsenic, and after that some ground glass." He also recalled that he had "injected live germs into a can of fish before presenting it to her."
Fortunately for Catherine, she survived the attempted murder, and she was ultimately saved from further assault when Hannah Peck came to town and became the center of Arthur Waite's attention. According to Waite, he started poisoning Hannah from the very first meal after she arrived. He gave her six assorted tubes of pneumonia, diphtheria, and influenza germs in her food and nasal spray. He also injected cultures into her mouth during a dental procedure. He recalled that "when she finally became ill and took to her bed, I ground up 12 five-grain veronal tablets (a barbiturate) and gave her that, too." Ultimately, it wasn't the germs that killed Hannah. It was the toxic veronal tablets, and possibly arsenic according to this report, that Waite had used to finish her off. She ultimately was said to have succumbed to kidney failure, which can be a side effect from both barbiturate and arsenic poisoning.
After successfully murdering Hannah Peck and then convincing the family to quickly cremate her body in order to cover up the evidence of poisoning, Arthur set his sights on the grieving husband and father. Acting as a caretaker, Waite testified that he used chlorine gas in his father-in-law's room in an attempt to make his throat more sensitive to the germ cultures. He would drive Joseph Peck around with open windows while keeping them raised in his bedroom as well during the cold winter nights in an unsuccessful bid to give the elder man pneumonia. After his failure to cause disease in John Peck with bacterial cultures and frigid winter air, Waite placed arsenic in his soup, tea and eggnog. Oddly enough, this measure also failed to kill John Peck. Thus, Arthur Waite resorted to chloroform and a pillow to finally suffocate him to death.
Fortunately, Arthur Waite did not get away with murder. While he tried once again to get the body swiftly cremated, his attempt was ultimately unsuccessful when a relative, who had spotted Waite going around town with a mistress, alerted the family to have an autopsy performed due to his suspicious behavior. The coroner found arsenic in John Peck's body, and it was revealed that Waite had tried to bribe the embalmer to put arsenic in the embalming fluid. Arthur Waite was convicted of murder and put to death by electric chair on May 25th, 1917. Had the germ "theory" actually worked as theorized, Waite would have easily gotten away with murder.
Poisoning the Pecks: New book details infamous 1916 Grand Rapids murder case"Once married, Waite began extensive attempts to poison the Pecks by first dosing mother-in-law Hannah Peck's food with a mixture of diphtheria and influenza germs. The scheme worked and the elderly woman fell ill and died in January 1916.
John Peck had a tougher constitution and Waite's attempts to dose him with illness-causing germs fell short. Finally, in March 1916, Waite resorted to arsenic-laced eggnog and finished his father-in-law off by suffocating the man with a pillow.
The plot occurred largely in New York, where Waite was using Peck family money to lead a double life with mistress Margaret Horton.
Had Waite successfully infected John Peck with an illness virulent enough to cause his death — he tried diphtheria, tuberculosis, typhus and influenza — he likely would have gotten away with the murders. But he couldn't get virulent enough germs and preserve them in a way that kept them dangerous, Buhk said.
Waite also tried to kill Peck's sister, Catherine, with germs.
"The depth of Waite's deception was shocking to people," said Buhk. Newspaper accounts of the time referred to the man's "tissue of lies."
Waite tried to have John Peck's body cremated quickly in order to destroy the evidence of arsenic poisoning. He'd managed it with Hannah Peck, but a friend of the family got suspicious after having watched both Pecks die in Waite's posh Manhattan apartment."
https://www.mlive.com/news/grand-rapids/2014/10/poisoning_the_pecks.html

While the spectacular failure of Arthur Waite to use "deadly germs" to kill his victims is compelling evidence, that is not the most incriminating demonstration against the germ "theory" of disease. In what is likely the most (in)famous failed attempt to prove the germ "theory" of disease, during the height of the most deadly "virus" of all time with the Spanish flu, researcher Milton Rosenau attempted to prove how the disease spread as well as identify a causative agent. To do so, volunteers at Gallops Island in Boston were subjected to one strain and then several strains of Pfeiffer's bacillus by spray and swab into their noses, throats and eyes. When these attempts failed to produce disease, new volunteers were inoculated with mixtures of other organisms isolated from the throats and noses of influenza patients. These attempts also failed, so the researchers used the blood from influenza patients and injected this into volunteers. When that failed to produce disease as well, thirteen volunteers were taken into an influenza ward and exposed to 10 influenza patients each. True to form, this final attempt also failed to produce disease. These same experiments were conducted on the other side of the continent at Goat Island in San Francisco, and the researchers obtained the exact same results. This left Rosenau confused, stating that they entered the experiments believing that they knew how disease spread from person to person. However, afterward, the researchers were left admitting that they knew absolutely nothing at all.
Experiments to Determine Mode of Spread of Influenza Milton J. Rosenau, M.D. Boston"Now, we proceeded rather cautiously at first by administering a pure culture of bacillus of influenza, Pfeiffer's bacillus, in a rather moderate amount, into the nostrils of a few of these volunteers. These early experiments I will not stop to relate, but I will go at once to what I may call our Experiment 1.
As the preliminary trials proved negative, we became bolder, and selecting nineteen of our volunteers, gave each one of them a very large quantity of a mixture of thirteen different strains of the Pfeiffer bacillus, some of them obtained recently from the lungs at necropsy; others were subcultures of varying age, and each of the thirteen had, of course, a different history. Suspensions of these organisms were sprayed with an atomizer into the nose and into the eyes, and back into the throat, while the volunteers were breathing in. We used some billions of these organisms, according to our estimated counts, on each one of the volunteers, but none of them took sick.
Then we proceeded to transfer the virus obtained from cases of the disease; that is, we collected the material and mucous secretions of the mouth and nose and throat and bronchi from cases of the disease and transferred this to our volunteers."
"In this particular experiment, in which we used ten volunteers, each of them received a comparatively small quantity of this, about 1 c.c. sprayed into each nostril and into the throat, while inspiring, and on the eye. None of these took sick. Some of the same material was filtered and instilled into other volunteers but produced no results."
"Now, thinking that perhaps the failure to reproduce the disease in the experiments that I have described was due to the fact that we obtained the material in the hospitals in Boston, and then took it down the bay to Gallops Island, which sometimes required four hours before our volunteers received the material, and believing that the virus was perhaps very frail, and could not stand this exposure, we planned another experiment, in which we obtained a large amount of material, and by special arrangements, rushed it down to Gallops Island; so that the interval between taking the material from the donors and giving it to our volunteers was only one hour and forty minutes, all told. Each one of these volunteers in this experiment, ten in number, received 6 c.c. of the mixed stuff that I have described. They received it into each nostril; received it in the throat, and on the eye; and when you think that 6 c.c. in all was used, you will understand that some of it was swallowed. None of them took sick."
"We used nineteen volunteers for this experiment, and it was during the time of the outbreak, when we had a choice of many donors. A few of the donors were in the first day of the disease. Others were in the second or third day of the disease. None of these volunteers who received the material thus directly transferred from cases took sick in any way. When I say none of them took sick in any way, I mean that after receiving the material they were then isolated on Gallops Island. Their temperature was taken three times a day and carefully examined, of course, and under constant medical supervision they were held for one full week before they were released, and perhaps used again for some other experiment. All of the volunteers received at least two, and some of them three "shots" as they expressed it.
Our next experiment consisted in injections of blood. We took five donors, five cases of influenza in the febrile stage, some of them again quite early in the disease. We drew 20 'c.c. from the arm vein of each, making a total of 100 c.c, which was mixed and treated with 1 per cent, of sodium citrate. Ten c.c. of the citrated whole blood were injected into each of the ten volunteers. None of them took sick in any way. Then we collected a lot of mucous material from the upper respiratory tract, and filtered it through Mandler filters. While these filters will hold back the bacteria of ordinary size, they will allow "ultramicroscopic" organisms to pass. This filtrate was injected into ten volunteers, each one receiving 3.5 c.c. subcutaneously, and none of these took sick in any way.
The next experiment was designed to imitate the natural way in which influenza spreads, at least the way in which we believe influenza spreads, and I have no doubt it does—by human contact. This experiment consisted in bringing ten of our volunteers from Gallops Island to the U.S. Naval Hospital at Chelsea, into a ward having thirty beds, all filled with influenza."
"I may say that the volunteers were perfectly splendid about carrying out the technic of these experiments. They did it with a high idealism. They were inspired with the thought that they might help others. They went through the program in a splendid spirit. After our volunteer had had this sort of contact with the patient, talking and chatting and shaking hands with him for five minutes, and receiving his breath five times, and then his cough five times directly in his face, he moved to the next patient whom we had selected, and repeated this, and so on, until this volunteer had had that sort of contact with ten different cases of influenza, in different stages of the disease, mostly fresh cases, none of them more than three days old.
We will remember that each one of the ten volunteers had that sort of intimate contact with each one of the ten different influenza patients. They were watched carefully for seven days—and none of them took sick in any way."
"Dr. McCoy, who with Dr. Richey, did a similar series of experiments on Goat Island, San Francisco, used volunteers who, so far as known, had not been exposed to the outbreak at all, also had negative results, that is, they were unable to reproduce the disease. Perhaps there are factors, or a factor, in the transmission of influenza that we do not know.
As a matter of fact, we entered the outbreak with a notion that we knew the cause of the disease, and were quite sure we knew how it was transmitted from person to person. Perhaps, if we have learned anything, it is that we are not quite sure what we know about the disease."
https://zenodo.org/record/1505669/files/article.pdf?download=1

As can be seen, there are numerous examples of researchers and volunteers (both willing and unwilling) who demonstrated the truth that pure cultures of so-called "pathogenic" bacteria did not live up to the deadly disease-producing reputation. However, even in the face of insurmountable evidence that the germs can not cause disease, some people are unwilling to give up their preconceived beliefs in order to look at the evidence logically. Thus, even though the proof against the germ "theory" was provided, they still feel the need to try and shift the burden of proof away from themselves to provide evidence supporting pathogenic bacteria in an attempt to place it on to those who have successfully challenged said claim. This is what happened to Dr. John Fraser, who is the Canadian doctor that was discussed at the start of this article. Even though he had over 5 years and 150 experiments demonstrating the inability of bacteria to cause disease, he was challenged to provide even more evidence supporting his claims. This came via a Minnesota doctor by the name of H. W. Hill who wanted Dr. Fraser to subject himself to even more experiments to prove his claims against germ "theory." At the time, Dr. Fraser was on vacation, and so in his stead, another doctor from Minnesota by the name of H.A. Zettel stepped up to take his place. However, Dr. Zettel challenged Dr. Hill to having them both submit to inoculation with the germs of typhoid, tuberculosis, diphtheria, meningitis, smallpox, and leprosy. During the challenge, Dr. Zettel would use only diet and general hygiene for "protection" while Dr. Hill would use anti-toxins and vaccines. Thus, a proper germ duel was established. Sadly, Dr. Hill did not accept the challenge, and the germ duel was never settled.
Beyond recounting these events, the article reprinted below has some rather startling admissions:
- There was a lack of success of the medical profession in trying to prevent and cure disease by treatments based on the germ "theory."
- The number of people who depended on drugless healing had been rapidly increasing.
- At the time, thirty-five million peopIe in the United States depended upon some form of drugless healing when sick.
- The average mortality from disease would not have been over 7 percent without any medical treatment, while the mortality under the treatment of some physicians was 12 percent.
- Mortality from the Spanish flu was 10 to 20 percent when treated by medical professionals, whereas it was less than 1 percent when people relied on natural healing.
Thus, it can be seen that it is not the germs, but rather the treatments themselves that lead to disease and death.
LET'S GET AT THE TRUTHA few months ago Dr. John B. Fraser of Toronto published 'an article describing extensive experiments which he had made to determine if germs cause disease or not, his conclusion being that they do not. He ended by challenging the medical profession to make similar experiments to test the germ theory. The matter was taken up by Dr. H. W. Hill of Minneapolis, who challenged Dr. Fraser to submit himself as the subject of the experiments. Dr. Fraser being then on his vacation, the challenge was accepted by Dr. H. A. Zettel of St. Paul, who suggested that both he and Dr. Hill should submit to inoculation with the germs of typhoid, tuberculosis, diphtheria, meningitis, smallpox and leprosy. Dr. Zettel was to rely on diet and general hygiene for protection against these diseases, while Dr. Hill would use anti-toxins and vaccines. Dr. Hill, however, did not accept the challenge and the "duel" still hangs fire. Legal experts say that if the plan were carried out and one of the doctors should die the other would be legally guilty of murder.
While the circumstances of this "germ duel" are rather amusing, it brings up a subjeet of vital importance, the correctness of the germ theory, according to a physician. As a result of the lack of success of the medical profession in trying to prevent and cure disease by treatments based on the germ theory, the number of people who depend on drugless healing is rapidly increasing. In an article in a medical magazine, Ely G. Jones, M. D., M Buffalo, recently said: "As physicians we have failed in our duty to the sick; we have failed to find a definite treatment for the diseases common to our coutry. As a result of this sad state things there are thirty-five million peopIe in the United States that depend upon some form of drugless healing when they are sick. It is said that 'the average mortality from disease in this country would not be over 7 percent without any medical treatment.' The mortality under the treatment of some physicians is 12 percent. From this it will be seen that the public would be better off without them. If we as physicians are to be of any real benefit to the public the mortality under our treatment must be below 7 percent."
It might be mentioned in connection with the above statement that the mortality from the flu during the epidemic was from 10 to 20 percent when treated by the regular medical methods, whereas it is claimed drugless methods of treatment resulted in a mortality of less than 1 percent.
It would seem that more conclusive proof of the germ theory is required than has yet been produced. For the benefit of humanity as well as in the interest of science, the medical .profession should perform experiments similar to Dr. Fraser's and those made by the government last winter when unsuccessful attempts were made to cause the flu by inoculation and voluntary exposure to contagion. If the germ theory is right the results of such experiments will prove it. And if it is wrong the sooner the world knows it the better.
-From the Rocky Mountain News, Denver, Colo., October 13, 1919, and Chicago Evening Post, October 21, 1919.
Click to access OsteopathicTruthVol4No3Oct1919.pdf
While Dr. Hill ultimately cowered in the face of the germ duel, even if he had accepted it, those in charge of keeping the germ "theory" narrative intact had a plan to discourage it from ever taking place. Had the challenge been accepted, it was decided that if anyone died as a result of the duel, the other participant would be charged with murder. This was obviously used to keep both men from participating in what would have most assuredly been another dark stain left upon the germ "theory" of disease.
MURDER CHARGE IF DUEL OF GERMS PROVES FATAL St. Paul Doctor's Challenge Has Not Been Answered Yet, However.ST. PAUL, July 17. Death, resulting from injection ot disease germs in the body, whether experimentally or otherwise, would be murder. Thls was the opinion to-day of Harry Peterson, assistant prosecuting attorney, regarding the "threat" of two physicians to inoculate each other with disease and use different methods of attempting to cure themselves.
Dr. H. W. Hill, who challenged Dr. John B. Fraser ot Toronto, said he had heard no more from the latter. In the meantime Dr. H. A. Zettel of St. Paul offered to take Dr. Fraser'a place, but was refused by Dr. Hill."
https://www.loc.gov/resource/sn83030193/1919-07-17/ed-1/?st=text&r=0.136,0.119,0.386,0.574,0

Albert Einstein once said that no amount of experimentation could ever prove him right, but a single experiment could prove him wrong. Those defending the germ "theory" of disease should take heed of his words. It does not matter how many papers filled with pseudoscientific experiments with unnatural exposure routes that they put forward. All it takes is a single well-done scientific experiment using natural exposure methods to falsify the hypothesis that germs cause disease. Unfortunately for those defending the germ "theory," there has not been just a single experiment that falsified the underlying hypothesis supporting the "theory," but a multitude of them that have shown that the most "deadly and dangerous" microbes cannot cause illness when healthy subjects are exposed. Thus, while the germ duel was not officially accepted by Dr. Hill in 1919, it had already been settled before the duel had ever begun. Due to the brave work of various researchers willing to question the authorities and the rising dogma, the germ "theory" of disease had been fatally shot down in a blaze of glory.
This article originally appeared on ViroLIEgy's Antiviral Substack.